

Characterization of static and dynamic left ventricular diastolic function in patients with heart failure with a preserved ejection fraction
- PMID: 20682947
- PMCID: PMC3716372
- DOI: 10.1161/CIRCHEARTFAILURE.109.867044
Characterization of static and dynamic left ventricular diastolic function in patients with heart failure with a preserved ejection fraction
Abstract
Background: Congestive heart failure in the setting of a preserved left ventricular (LV) ejection fraction is increasing in prevalence among the senior population. The underlying pathophysiologic abnormalities in ventricular function and structure remain unclear for this disorder. We hypothesized that patients with heart failure with preserved ejection fraction (HFPEF) would have marked abnormalities in LV diastolic function with increased static diastolic stiffness and slowed myocardial relaxation compared with age-matched healthy controls.
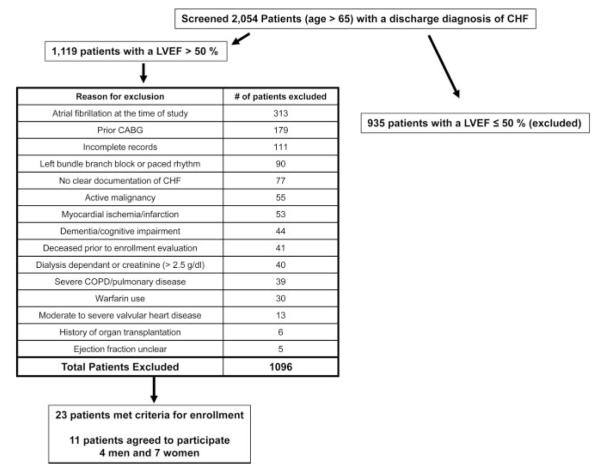
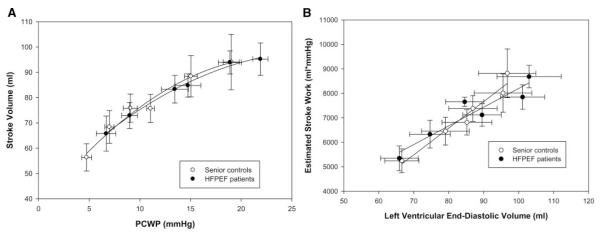
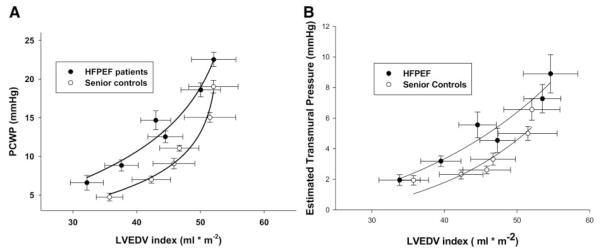
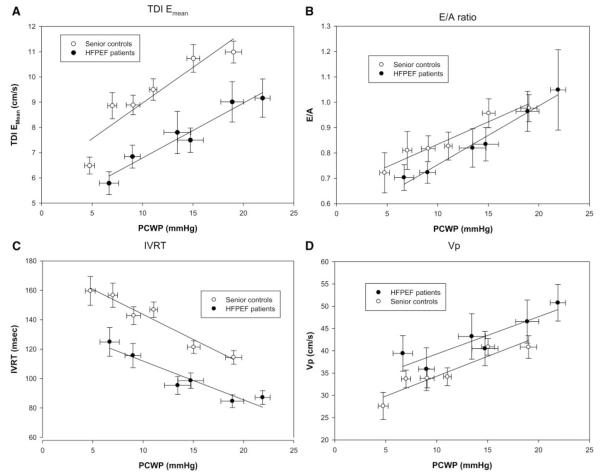
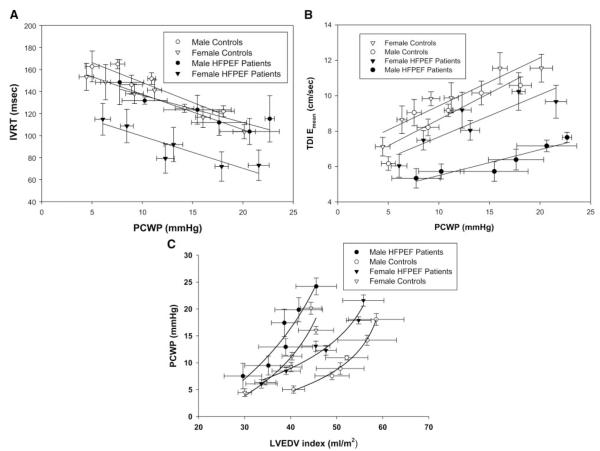
Methods and results: Eleven highly screened patients (4 men, 7 women) aged 73±7 years with HFPEF were recruited to participate in this study. Thirteen sedentary healthy controls (7 men, 6 women) aged 70±4 years also were recruited. All subjects underwent pulmonary artery catheterization with measurement of cardiac output, end-diastolic volumes, and pulmonary capillary wedge pressures at baseline; cardiac unloading (lower-body negative pressure or upright tilt); and cardiac loading (rapid saline infusion). The data were used to define the Frank-Starling and LV end-diastolic pressure-volume relationships. Doppler echocardiographic data (tissue Doppler velocities, isovolumic relaxation time, propagation velocity of early mitral inflow , E/A-wave ratio) were obtained at each level of cardiac preload. Compared with healthy controls, patients with HFPEF had similar LV contractile function and static LV compliance but reduced LV chamber distensibility with elevated filling pressures and slower myocardial relaxation as assessed by tissue Doppler imaging.
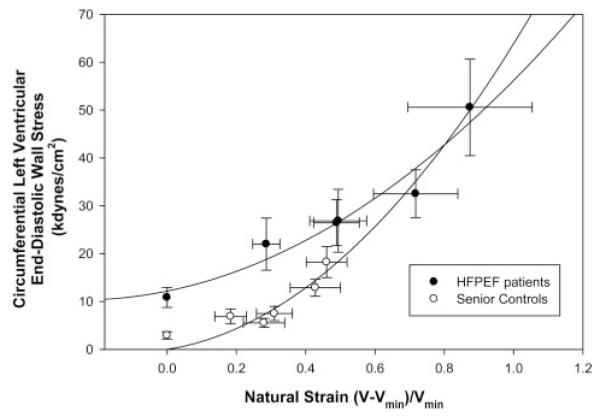
Conclusions: In this small, highly screened patient population with hemodynamically confirmed HFPEF, increased end-diastolic static ventricular stiffness relative to age-matched controls was not a universal finding. Nevertheless, patients with HFPEF, even when well compensated, had elevated filling pressures, reduced distensibility, and increased diastolic wall stress compared with controls. In contrast, LV relaxation as assessed by tissue Doppler variables appeared consistently impaired in patients with HFPEF.
Figures
References
-
- Kitzman DW, Daniel KR. Diastolic heart failure in the elderly. Clin Geriatr Med. 2007;23:83–106. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Prasad A, Levine BD. Aging and diastolic heart failure. In: Klein A, Garcia M, editors. Diastology. Elsevier; Philadelphia: 2008.
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure–abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350:1953–1959. - PubMed
-
- Arbab-Zadeh A, Dijk E, Prasad A, Fu Q, Torres P, Zhang R, Thomas JD, Palmer D, Levine BD. Effect of aging and physical activity on left ventricular compliance. Circulation. 2004;110:1799–1805. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
