

Temporal changes in programme outcomes among adult patients initiating antiretroviral therapy across South Africa, 2002-2007
- PMID: 20683318
- PMCID: PMC2948209
- DOI: 10.1097/QAD.0b013e32833d45c5
Temporal changes in programme outcomes among adult patients initiating antiretroviral therapy across South Africa, 2002-2007
Abstract
Objective: Little is known about the temporal impact of the rapid scale-up of large antiretroviral therapy (ART) services on programme outcomes. We describe patient outcomes [mortality, loss-to-follow-up (LTFU) and retention] over time in a network of South African ART cohorts.
Design: Cohort analysis utilizing routinely collected patient data.
Methods: Analysis included adults initiating ART in eight public sector programmes across South Africa, 2002-2007. Follow-up was censored at the end of 2008. Kaplan-Meier methods were used to estimate time to outcomes, and proportional hazards models to examine independent predictors of outcomes.
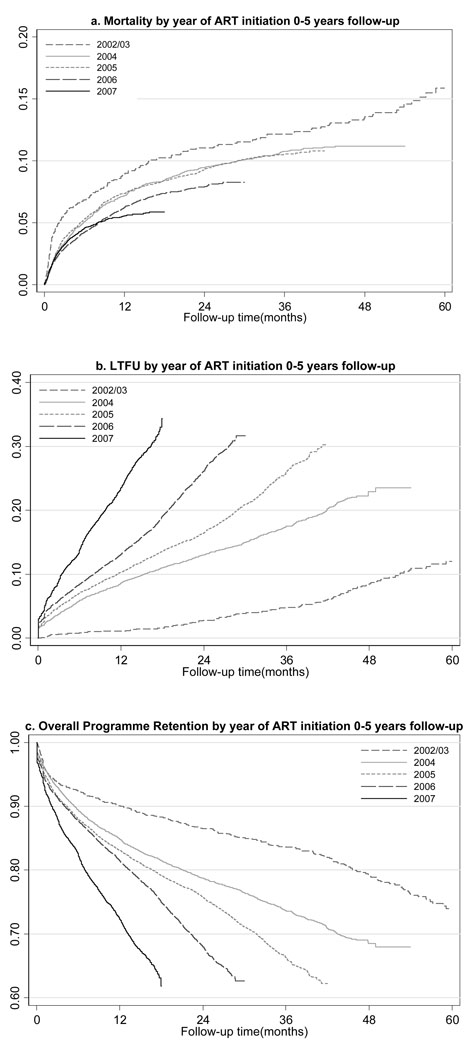
Results: Enrolment (n = 44 177, mean age 35 years; 68% women) increased 12-fold over 5 years, with 63% of patients enrolled in the past 2 years. Twelve-month mortality decreased from 9% to 6% over 5 years. Twelve-month LTFU increased annually from 1% (2002/2003) to 13% (2006). Cumulative LTFU increased with follow-up from 14% at 12 months to 29% at 36 months. With each additional year on ART, failure to retain participants was increasingly attributable to LTFU compared with recorded mortality. At 12 and 36 months, respectively, 80 and 64% of patients were retained.
Conclusion: Numbers on ART have increased rapidly in South Africa, but the programme has experienced deteriorating patient retention over time, particularly due to apparent LTFU. This may represent true loss to care, but may also reflect administrative error and lack of capacity to monitor movements in and out of care. New strategies are needed for South Africa and other low-income and middle-income countries to improve monitoring of outcomes and maximize retention in care with increasing programme size.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- World Health Organization, UNAIDS, UNICEF. Towards Universal Access: Scaling up Priority HIV/AIDS Interventions in the Health Sector: Progress Report. Geneva: WHO; 2007.
-
- Department of Health. Progress Report on Declaration of Commitment on HIV and AIDS: Republic of South Africa: Reporting Period: January 2006 – December 2007. 2008.
-
- Cornell M, Technau K, Fairall LR, Wood R, Moultrie H, Van Cutsem G, et al. Monitoring the South African National Antiretroviral Treatment Programme, 2003 – 2007: The IeDEA Southern Africa Collaboration. South African Medical Journal. 2009. pp. 653–660. Full text available at: http://www.samj.org.za/index.php/samj/article/viewFile/3437/2485. - PMC - PubMed
-
- Zachariah R, Harries K, Moses M, Manzi M, Line A, Mwagomba B, Harries AD. Very early mortality in patients starting antiretroviral treatment aqt primary health centres in rural Malawi. Trop Med Int Health. 2009;14:713–721. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
