

Congenital generalized lipodystrophy, type 4 (CGL4) associated with myopathy due to novel PTRF mutations
- PMID: 20684003
- PMCID: PMC2930069
- DOI: 10.1002/ajmg.a.33578
Congenital generalized lipodystrophy, type 4 (CGL4) associated with myopathy due to novel PTRF mutations
Abstract
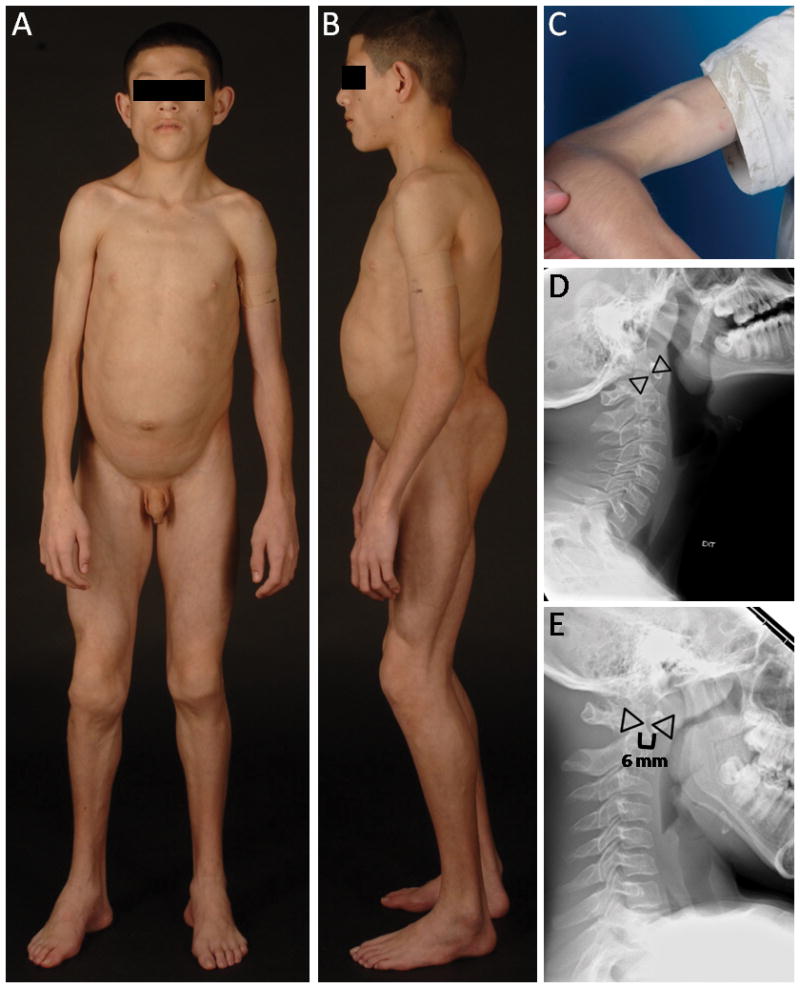
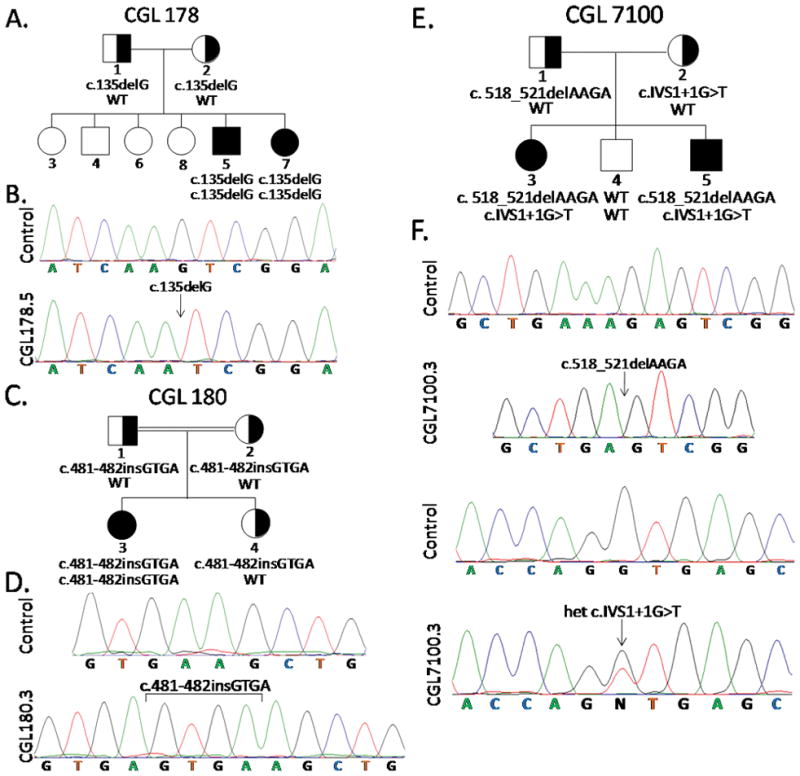
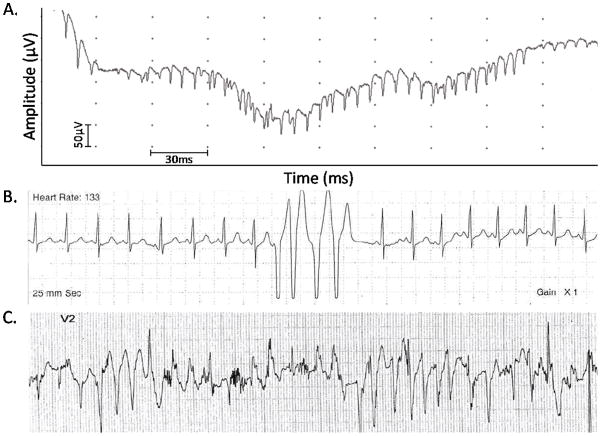
Congenital generalized lipodystrophy (CGL) is a rare autosomal recessive disorder characterized by near total absence of body fat since birth with predisposition to insulin resistance, diabetes, hypertriglyceridemia, and hepatic steatosis. Three CGL loci, AGPAT2, BSCL2, and CAV1, have been identified previously. Recently, mutations in polymerase I and transcript release factor (PTRF) were reported in five Japanese patients presenting with myopathy and CGL (CGL4). We report novel PTRF mutations and detailed phenotypes of two male and three female patients with CGL4 belonging to two pedigrees of Mexican origin (CGL7100 and CGL178) and one pedigree of Turkish origin (CGL180). All patients had near total loss of body fat and congenital myopathy manifesting as weakness, percussion-induced muscle mounding, and high serum creatine kinase levels. Four of them had hypertriglyceridemia. Three of them had atlantoaxial instability. Two patients belonging to CGL178 pedigree required surgery for pyloric stenosis in the first month of life. None of them had prolonged QT interval on electrocardiography but both siblings belonging to CGL7100 had exercise-induced ventricular arrhythmias. Three of them had mild acanthosis nigricans but had normal glucose tolerance. Two of them had hepatic steatosis. All patients had novel null mutations in PTRF gene. In conclusion, mutations in PTRF result in a novel phenotype that includes generalized lipodystrophy with mild metabolic derangements, myopathy, cardiac arrhythmias, atlantoaxial instability, and pyloric stenosis. It is unclear how mutations in PTRF, which plays an essential role in formation of caveolae, affect a wide variety of tissues resulting in a variable phenotype.
Copyright 2010 Wiley-Liss, Inc.
Figures
Similar articles
-
Novel PTRF mutation in a child with mild myopathy and very mild congenital lipodystrophy.BMC Med Genet. 2013 Sep 11;14:89. doi: 10.1186/1471-2350-14-89. BMC Med Genet. 2013. PMID: 24024685 Free PMC article.
-
Fatal cardiac arrhythmia and long-QT syndrome in a new form of congenital generalized lipodystrophy with muscle rippling (CGL4) due to PTRF-CAVIN mutations.PLoS Genet. 2010 Mar 12;6(3):e1000874. doi: 10.1371/journal.pgen.1000874. PLoS Genet. 2010. PMID: 20300641 Free PMC article.
-
Congenital generalized lipodystrophy type 4 due to a novel PTRF/CAVIN1 pathogenic variant in a child: effects of metreleptin substitution.J Pediatr Endocrinol Metab. 2022 Apr 11;35(7):946-952. doi: 10.1515/jpem-2022-0022. Print 2022 Jul 26. J Pediatr Endocrinol Metab. 2022. PMID: 35405042
-
A new mutation in the CAVIN1/PTRF gene in two siblings with congenital generalized lipodystrophy type 4: case reports and review of the literature.Front Endocrinol (Lausanne). 2023 Jul 12;14:1212729. doi: 10.3389/fendo.2023.1212729. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37501786 Free PMC article. Review.
-
Congenital generalized lipodystrophies--new insights into metabolic dysfunction.Nat Rev Endocrinol. 2015 Sep;11(9):522-34. doi: 10.1038/nrendo.2015.123. Epub 2015 Aug 4. Nat Rev Endocrinol. 2015. PMID: 26239609 Free PMC article. Review.
Cited by
-
Human adipose dynamics and metabolic health.Ann N Y Acad Sci. 2013 Apr;1281(1):160-77. doi: 10.1111/nyas.12009. Epub 2013 Jan 14. Ann N Y Acad Sci. 2013. PMID: 23317303 Free PMC article. Review.
-
Determining residual adipose tissue characteristics with MRI in patients with various subtypes of lipodystrophy.Diagn Interv Radiol. 2017 Nov-Dec;23(6):428-434. doi: 10.5152/dir.2017.17019. Diagn Interv Radiol. 2017. PMID: 29044029 Free PMC article.
-
Muscular dystrophy in PTFR/cavin-1 null mice.JCI Insight. 2017 Mar 9;2(5):e91023. doi: 10.1172/jci.insight.91023. JCI Insight. 2017. PMID: 28289716 Free PMC article.
-
Approach to Diagnosing a Pediatric Patient With Severe Insulin Resistance in Low- or Middle-income Countries.J Clin Endocrinol Metab. 2021 Nov 19;106(12):3621-3633. doi: 10.1210/clinem/dgab549. J Clin Endocrinol Metab. 2021. PMID: 34318892 Free PMC article.
-
Fat caves: caveolae, lipid trafficking and lipid metabolism in adipocytes.Trends Endocrinol Metab. 2011 Aug;22(8):318-24. doi: 10.1016/j.tem.2011.04.001. Epub 2011 May 17. Trends Endocrinol Metab. 2011. PMID: 21592817 Free PMC article. Review.
References
-
- Agarwal AK, Simha V, Oral EA, Moran SA, Gorden P, O’Rahilly S, Zaidi Z, Gurakan F, Arslanian SA, Klar A, Ricker A, White NH, Bindl L, Herbst K, Kennel K, Patel SB, Al-Gazali L, Garg A. Phenotypic and genetic heterogeneity in congenital generalized lipodystrophy. J Clin Endocrinol Metab. 2003;88:4840–4847. - PubMed
-
- Antuna-Puente B, Boutet E, Vigouroux C, Lascols O, Slama L, Caron-Debarle M, Khallouf E, Levy-Marchal C, Capeau J, Bastard JP, Magre J. Higher adiponectin levels in patients with Berardinelli-Seip congenital lipodystrophy due to seipin as compared with 1-acylglycerol-3-phosphate-o-acyltransferase-2 deficiency. J Clin Endocrinol Metab. 95:1463–1468. - PubMed
-
- Barbuti A, Terragni B, Brioschi C, DiFrancesco D. Localization of f-channels to caveolae mediates specific beta2-adrenergic receptor modulation of rate in sinoatrial myocytes. J Mol Cell Cardiol. 2007;42:71–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
