

An interactive surgical planning tool for acetabular fractures: initial results
- PMID: 20684761
- PMCID: PMC2923114
- DOI: 10.1186/1749-799X-5-50
An interactive surgical planning tool for acetabular fractures: initial results
Abstract
Background: Acetabular fractures still are among the most challenging fractures to treat because of complex anatomy, involved surgical access to fracture sites and the relatively low incidence of these lesions. Proper evaluation and surgical planning is necessary to achieve anatomic reduction of the articular surface and stable fixation of the pelvic ring. The goal of this study was to test the feasibility of preoperative surgical planning in acetabular fractures using a new prototype planning tool based on an interactive virtual reality-style environment.
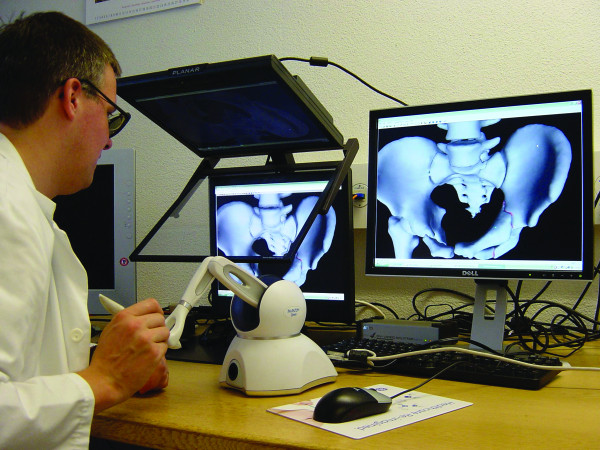
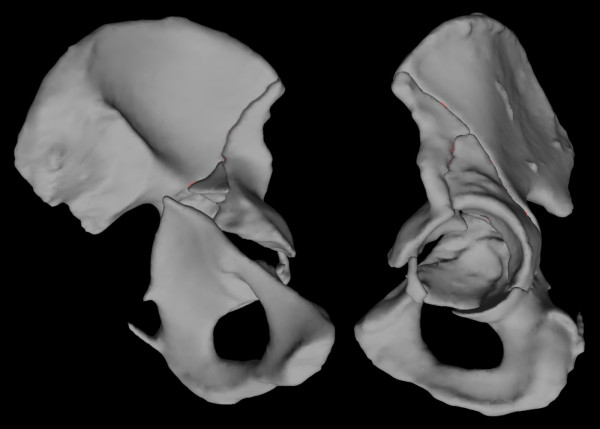
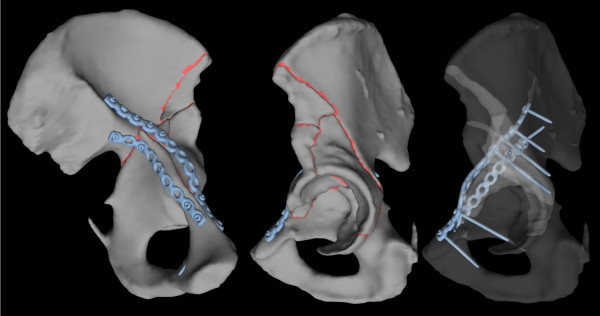
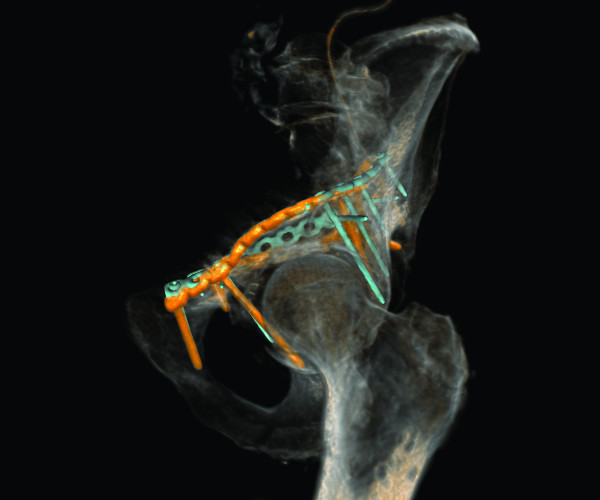
Methods: 7 patients (5 male and 2 female; median age 53 y (25 to 92 y)) with an acetabular fracture were prospectively included. Exclusion criterions were simple wall fractures, cases with anticipated surgical dislocation of the femoral head for joint debridement and accurate fracture reduction. According to the Letournel classification 4 cases had two column fractures, 2 cases had anterior column fractures and 1 case had a T-shaped fracture including a posterior wall fracture.The workflow included following steps: (1) Formation of a patient-specific bone model from preoperative computed tomography scans, (2) interactive virtual fracture reduction with visuo-haptic feedback, (3) virtual fracture fixation using common osteosynthesis implants and (4) measurement of implant position relative to landmarks. The surgeon manually contoured osteosynthesis plates preoperatively according to the virtually defined deformation. Screenshots including all measurements for the OR were available.The tool was validated comparing the preoperative planning and postoperative results by 3D-superimposition.
Results: Preoperative planning was feasible in all cases. In 6 of 7 cases superimposition of preoperative planning and postoperative follow-up CT showed a good to excellent correlation. In one case part of the procedure had to be changed due to impossibility of fracture reduction from an ilioinguinal approach. In 3 cases with osteopenic bone patient-specific prebent fixation plates were helpful in guiding fracture reduction. Additionally, anatomical landmark based measurements were helpful for intraoperative navigation.
Conclusion: The presented prototype planning tool for pelvic surgery was successfully integrated in a clinical workflow to improve patient-specific preoperative planning, giving visual and haptic information about the injury and allowing a patient-specific adaptation of osteosynthesis implants to the virtually reduced pelvis.
Figures






References
LinkOut - more resources
Full Text Sources
Other Literature Sources
