

Treatment options for patients with chronic myeloid leukemia who are resistant to or unable to tolerate imatinib
- PMID: 20685492
- PMCID: PMC4086628
- DOI: 10.1016/j.clinthera.2010.05.003
Treatment options for patients with chronic myeloid leukemia who are resistant to or unable to tolerate imatinib
Abstract
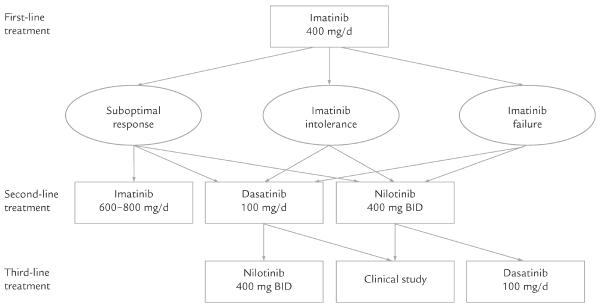
Background: Imatinib has been found to substantially improve outcomes in patients with chronic myeloid leukemia (CML) compared with previously available therapies. However, its use is complicated by development of resistance or drug intolerance, prompting dose escalation or a trial of dasatinib or nilotinib, the second-generation tyrosine kinase inhibitors (TKIs).
Objectives: This article reviews the mechanisms of TKI resistance; discusses the tolerability and efficacy of high-dose imatinib, dasatinib, and nilotinib; and provides background for the rational use of second-line treatment options.
Methods: MEDLINE (1966-December 2009) and EMBASE (1993-December 2009) were searched for pertinent English-language publications using search terms that included, but were not limited to, chronic myeloid leukemia, imatinib, dasatinib, nilotinib, and clinical trial. Abstracts from American Society of Hematology annual meetings (2005-2009) were also reviewed. There were no prespecified inclusion or exclusion criteria.
Results: Major and complete cytogenetic responses (MCyR and CCyR, respectively) to second-line treatment with high-dose (600-800 mg/d PO) imatinib were restricted to CML patients who had achieved a CyR to standard-dose imatinib: >90% of patients without a previous CyR failed to respond. The expected durability of the response to this approach remains unclear. Grade 3/4 thrombocytopenia, neutropenia, and anemia occurred in 14%, 39%, and 8%, respectively, of patients receiving high-dose imatinib. In patients who failed first-line treatment with imatinib, dasatinib (70 mg BID PO) was associated with higher rates of CCyR at 2 years compared with imatinib (44% vs 18%, respectively; P = 0.003), as well as higher estimated rates of progression-free survival at 2 years (86% vs 65%; P = 0.001). Dasatinib use was complicated by grade 3/4 thrombocytopenia and neutropenia in 57% and 63% of patients, respectively, and pleural effusion in 5%. Nilotinib treatment was effective in patients who were resistant to or unable to tolerate imatinib, with 46% and 58% achieving a CCyR and MCyR, respectively, at 2 years. Nilotinib use was complicated by grade 3/4 thrombocytopenia and neutropenia in 28% and 40% of patients, respectively, and QTc-interval prolongation in 1% to 10% of patients. Neither agent was clinically effective in patients with the common T315I mutation.
Conclusion: Dasatinib and nilotinib were effective and generally well tolerated as second-line treatments for CML patients with a suboptimal response to standard doses of imatinib or imatinib intolerance.
Copyright 2010 Excerpta Medica Inc. All rights reserved.
Figures
Similar articles
-
Dasatinib: from treatment of imatinib-resistant or -intolerant patients with chronic myeloid leukemia to treatment of patients with newly diagnosed chronic phase chronic myeloid leukemia.Clin Ther. 2012 Feb;34(2):272-81. doi: 10.1016/j.clinthera.2012.01.009. Epub 2012 Jan 27. Clin Ther. 2012. PMID: 22285209 Review.
-
Dasatinib induces durable cytogenetic responses in patients with chronic myelogenous leukemia in chronic phase with resistance or intolerance to imatinib.Leukemia. 2008 Jun;22(6):1200-6. doi: 10.1038/leu.2008.84. Epub 2008 Apr 10. Leukemia. 2008. PMID: 18401416
-
[Efficacy of dasatinib in treatment of imatinib-resistant BCR/ABL positive leukemia].Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2013 Jun;21(3):581-6. doi: 10.7534/j.issn.1009-2137.2013.03.009. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2013. PMID: 23815902 Chinese.
-
Optimizing therapy for patients with chronic myelogenous leukemia in chronic phase.Cancer. 2010 Mar 15;116(6):1419-30. doi: 10.1002/cncr.24928. Cancer. 2010. PMID: 20120030 Review.
-
Improving frontline treatment for chronic myeloid leukemia: emerging evidence for use of nilotinib and dasatinib.Clin Adv Hematol Oncol. 2011 Oct;9(10):734-45. Clin Adv Hematol Oncol. 2011. PMID: 22252576 Review.
Cited by
-
Update: the status of clinical trials with kinase inhibitors in thyroid cancer.J Clin Endocrinol Metab. 2014 May;99(5):1543-55. doi: 10.1210/jc.2013-2622. Epub 2014 Jan 13. J Clin Endocrinol Metab. 2014. PMID: 24423326 Free PMC article. Review.
-
Tyrosine kinase inhibitors induced immune thrombocytopenia in chronic myeloid leukemia?Hematol Rep. 2011 Oct 19;3(3):e29. doi: 10.4081/hr.2011.e29. Epub 2011 Dec 6. Hematol Rep. 2011. PMID: 22593820 Free PMC article.
-
Long lasting complete molecular remission after suspending dasatinib treatment in chronic myeloid leukemia.Exp Hematol Oncol. 2012 Jul 11;1(1):17. doi: 10.1186/2162-3619-1-17. Exp Hematol Oncol. 2012. PMID: 23210842 Free PMC article.
-
Omics and therapy - a basis for precision medicine.Mol Oncol. 2012 Apr;6(2):128-39. doi: 10.1016/j.molonc.2012.02.009. Epub 2012 Mar 8. Mol Oncol. 2012. PMID: 22445068 Free PMC article. Review.
-
Deciphering the scalene association among type-2 diabetes mellitus, prostate cancer, and chronic myeloid leukemia via enrichment analysis of disease-gene network.Cancer Med. 2019 May;8(5):2268-2277. doi: 10.1002/cam4.1845. Epub 2019 Apr 1. Cancer Med. 2019. PMID: 30938105 Free PMC article.
References
-
- Sawyers CL. Chronic myeloid leukemia. N Engl J Med. 1999;340:1330–1340. - PubMed
-
- Nowell PC, Hungerford DA. A minute chromosome in human chronic granulocytic leukemia. Science. 1960;132:1497. - PubMed
-
- Rowley JD. Letter: A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature. 1973;243:290–293. - PubMed
-
- Bartram CR, de Klein A, Hagemeijer A, et al. Translocation of c-ab1 oncogene correlates with the presence of a Philadelphia chromosome in chronic myelocytic leukaemia. Nature. 1983;306:277–280. - PubMed
-
- Groffen J, Stephenson JR, Heisterkamp N, et al. Philadelphia chromosomal breakpoints are clustered within a limited region, bcr, on chromosome 22. Cell. 1984;36:93–99. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
