

Circulating levels of soluble klotho and FGF23 in X-linked hypophosphatemia: circadian variance, effects of treatment, and relationship to parathyroid status
- PMID: 20685863
- PMCID: PMC2968736
- DOI: 10.1210/jc.2010-0589
Circulating levels of soluble klotho and FGF23 in X-linked hypophosphatemia: circadian variance, effects of treatment, and relationship to parathyroid status
Abstract
Context: Circulating fibroblast growth factor (FGF)-23 is variably elevated in individuals with X-linked hypophosphatemia (XLH), and klotho has recently been shown to effect renal phosphate handling, yet limited data are available on circulating FGF23 and klotho in XLH.
Objective: The objective of the study was to characterize circulating FGF23 and klotho in XLH.
Design: Children and adults with XLH withheld medication for 14 d. Fasting serum FGF23, PTH, klotho, phosphate, and 1,25 dihydroxyvitamin D were obtained. Treated adults were also sampled, and circadian sampling was performed in selected individuals.
Setting: The study was conducted at a hospital research unit at an academic medical center.
Patients and other participants: Participants included 23 individuals with XLH and eight controls.
Interventions: There were no interventions.
Main outcome measures: Serum klotho and FGF23 were measured.
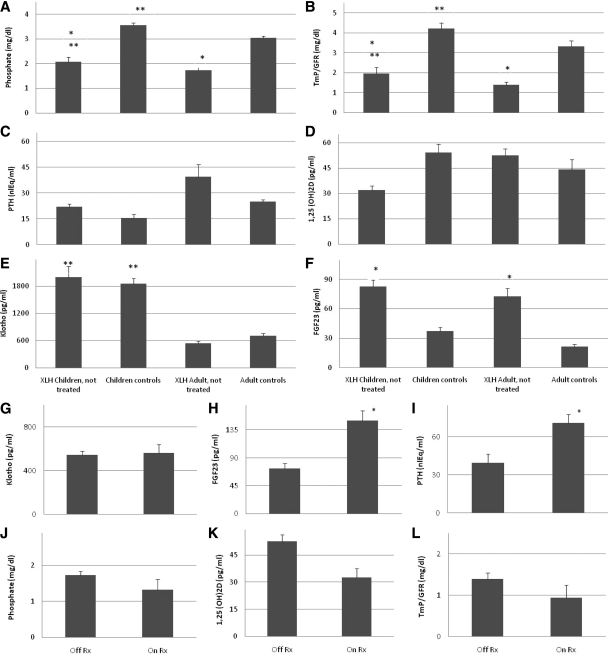
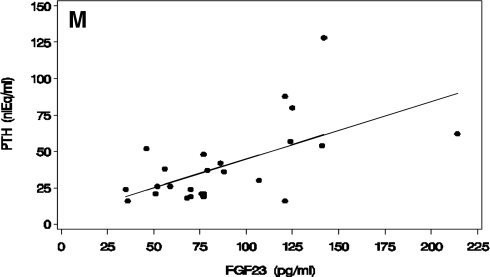
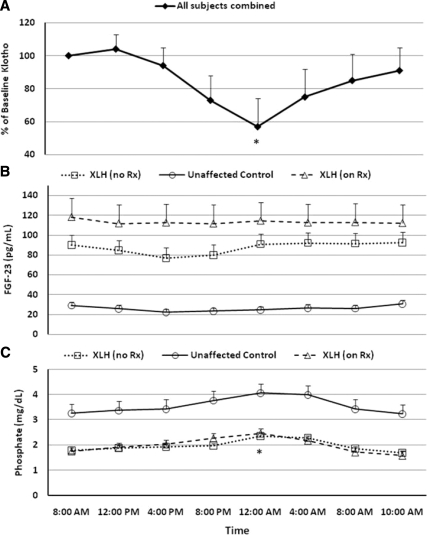
Results: FGF23 was greater in XLH than in controls and greater in treated XLH subjects compared with XLH subjects not receiving medical therapy. Children had higher klotho levels than adults, but values in XLH were similar to controls. A strong positive correlation between FGF23 and PTH was found in XLH subjects, whereas there was no relationship between these variables in controls. Circulating klotho, but not FGF23, has a diurnal pattern.
Conclusions: Serum klotho declines with age and demonstrates circadian variation but is normal in XLH. Serum FGF23 is similar in children and adults, is elevated in XLH, further increases with therapy, and demonstrates no diurnal variation. The direct relationship between FGF23 and PTH in subjects with XLH suggests that FGF23 regulation of PTH secretion is aberrant in this disorder.
Figures
References
-
- Carpenter TO, Drezner M 2007 Primary disorders of phosphate metabolism. In: Arnold A, section ed. (www.endotext.org, version of September 10, 2007). South Dartmouth, MA: mdtext.com, inc.
-
- Carpenter TO, Mitnick MA, Ellison A, Smith C, Insogna KL 1994 Nocturnal hyperparathyroidism: a frequent feature of X-linked hypophosphatemia. J Clin Endocrinol Metab 78:1378–1383 - PubMed
-
- Jonsson KB, Zahradnik R, Larsson T, White KE, Sugimoto T, Imanishi Y, Yamamoto T, Hampson G, Koshiyama H, Ljunggren O, Oba K, Yang IM, Miyauchi A, Econs MJ, Lavigne J, Jüppner H 2003 Fibroblast growth factor 23 in oncogenic osteomalacia and X-linked hypophosphatemia. N Engl J Med 348:1656–1663 - PubMed
-
- Carpenter TO 2003 Oncogenic osteomalacia—a complex dance of factors. N Engl J Med 348:1705–1708 - PubMed
-
- White KE, Carn G, Lorenz-Depiereux B, Benet-Pages A, Strom TM, Econs MJ 2001 Autosomal-dominant hypophosphatemic rickets (ADHR) mutations stabilize FGF-23. Kidney Int 60:2079–2086 - PubMed
