

Computed tomography-based structural analysis for predicting fracture risk in children with benign skeletal neoplasms: comparison of specificity with that of plain radiographs
- PMID: 20686056
- PMCID: PMC2909715
- DOI: 10.2106/JBJS.I.00871
Computed tomography-based structural analysis for predicting fracture risk in children with benign skeletal neoplasms: comparison of specificity with that of plain radiographs
Abstract
Background: The decision whether to treat benign skeletal lesions surgically can be difficult to make. The purpose of this study was to validate our previously published method of predicting fracture risk with use of quantitative computed tomography-based structural analysis.
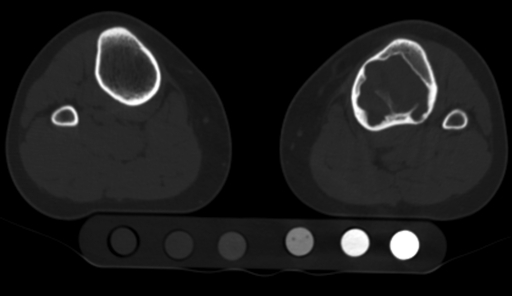
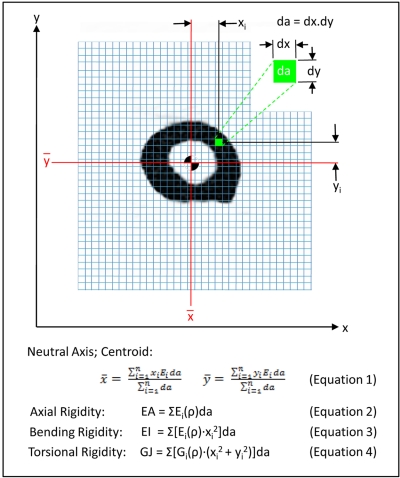
Methods: We prospectively studied a group of children who presented to a major children's hospital with a benign appendicular skeletal lesion between 2002 and 2007. As in our previous study, the resistance of the affected bone to compressive, bending, and torsional loads was calculated with rigidity analysis performed with the use of serial transaxial quantitative computed tomography data obtained along the length of the bone containing the lesion and from homologous cross sections through the contralateral, normal bone. At each cross section, the ratio of the structural rigidity of the affected bone to that of the normal, contralateral bone was determined.
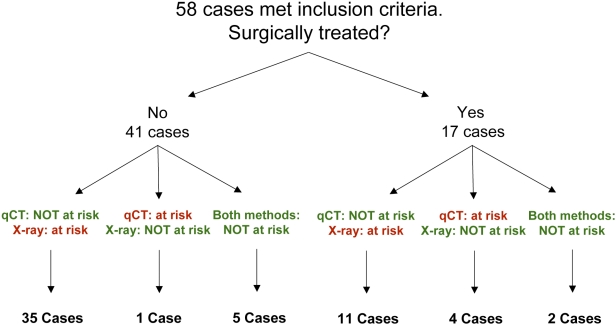
Results: Forty-one patients who had not received surgical treatment for the skeletal lesion met the criteria for our study. Thirty-four (83%) of these individuals completed our activity questionnaire at least two years after the quantitative computed tomography-based rigidity analysis. None of the patients for whom no increased fracture risk had been predicted by the rigidity analysis sustained a fracture, even though they had not received surgical treatment.
Conclusions: Many considerations other than the predicted fracture risk are factored into the decision of whether to treat a benign skeletal lesion. However, this study indicated that quantitative computed tomography-based rigidity analysis is more specific (97% specificity) than criteria based on plain radiographs (12% specificity) for predicting the risk of a pathologic fracture since fracture risk indices based on lesion size alone fail to account for the compensatory remodeling of the host bone that occurs in response to the presence of the lesion in a growing child.
Level of evidence: Prognostic Level I. See Instructions to Authors for a complete description of levels of evidence.
Figures
References
-
- Aboulafia AJ, Kennon RE, Jelinek JS. Begnign bone tumors of childhood. J Am Acad Orthop Surg. 1999;7:377-88 - PubMed
-
- Dormans JP, Flynn JM. Pathologic fractures associated with tumors and unique conditions of the musculoskeletal system. : Beaty JH, Kasser JR, Rockwood and Wilkins’ fractures in children. Vol 3 5th ed Philadelphia: Lippincott Williams and Wilkins; 2001. p 139-240
-
- Adler CP. Solid aneurysmal bone cyst with pathologic bone fracture. Skeletal Radiol. 1995;24:214-6 - PubMed
-
- Gitelis S, Wilkins R, Conrad EU., 2nd Benign bone tumors. Instr Course Lect. 1996;45:425-46 - PubMed
-
- Bitzan P, Windhager R, Lang S, Richling B, Kotz R. [Incidence of recurrence of aneurysmal bone cysts following surgical treatment and adjuvant therapy with phenol]. Z Orthop Ihre Grenzgeb. 1995;133:422-8 German - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
