

Relapse prevention in schizophrenia and schizoaffective disorder with risperidone long-acting injectable vs quetiapine: results of a long-term, open-label, randomized clinical trial
- PMID: 20686456
- PMCID: PMC3055334
- DOI: 10.1038/npp.2010.111
Relapse prevention in schizophrenia and schizoaffective disorder with risperidone long-acting injectable vs quetiapine: results of a long-term, open-label, randomized clinical trial
Erratum in
- Neuropsychopharmacology. 2011 Jan;36(2):548
Abstract
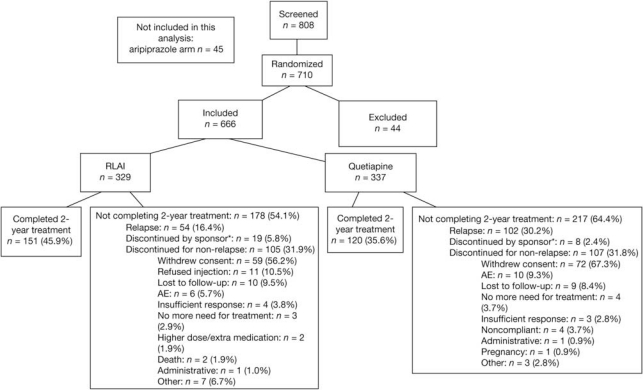
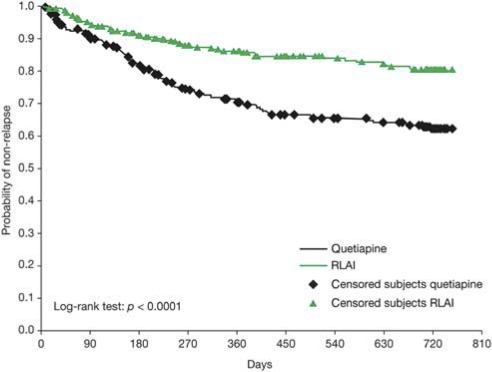
Chronic management of schizophrenia and schizoaffective disorders is frequently complicated by symptomatic relapse. An open-label, randomized, active-controlled, 2-year trial evaluated 710 patients with schizophrenia or related disorders who were switched from stable treatment with oral risperidone, olanzapine, or conventional neuroleptics to risperidone long-acting injectable (RLAI) or oral quetiapine. Primary effectiveness evaluation was time-to-relapse. Safety evaluations included adverse events (AEs) reported for the duration of the study, Extrapyramidal Symptom Rating Scale (ESRS), clinical laboratory tests, and vital signs. A total of 666 patients (n=329 RLAI, n=337 quetiapine) were evaluable for effectiveness measures. Baseline demographics were similar between treatment groups. Kaplan-Meier estimate of time-to-relapse was significantly longer with RLAI (p<0.0001). Relapse occurred in 16.5% of patients with RLAI and 31.3% with quetiapine. RLAI and quetiapine were both safe and well tolerated. Weight gain affected 7% of patients with RLAI and 6% with quetiapine, with mean end point increases of 1.25±6.61 and 0±6.55 kg, respectively. There were no significant between-group differences in weight gain. ESRS total scores decreased similarly after randomization to either RLAI or quetiapine. Extrapyramidal AEs occurred in 10% of patients with RLAI and 6% with quetiapine. Treatment-emergent potentially prolactin-related AEs were reported in 15 (5%) patients with RLAI and 5 (2%) patients with quetiapine; hyperprolactinemia was reported in 43 (13.1%) patients with RLAI and 5 (1.5%) patients with quetiapine. Somnolence occurred in 2% of patients with RLAI and 11% with quetiapine. To our knowledge, this is the first report of a randomized clinical trial directly comparing relapse prevention with a second-generation long-acting injectable antipsychotic and oral therapy. Time-to-relapse in stable patients with schizophrenia or schizoaffective disorder was significantly longer in patients randomized to RLAI compared with those randomized to oral quetiapine. Both antipsychotics were generally well tolerated.
Figures
References
-
- Acosta FJ, Bosch E, Sarniento G, Juanes N, Caballero-Hidalgo A, Mayans T. Evaluation of noncompliance in schizophrenia patients using electronic monitoring (MEMS(R)) and its relationship to sociodemographic, clinical and psychopathological variables. Schizophr Res. 2009;107:213–217. - PubMed
-
- American Psychiatric Association 1994Diagnostic and Statistical Manual of Mental Disorders4th edn.American Psychiatric Association: Washington, DC
-
- Chouinard G, Margolese HC. Manual for the Extrapyramidal Symptom Rating Scale (ESRS) Schizophr Res. 2005;76:247–265. - PubMed
-
- Chouinard G, Ross-Chouinard A, Annable L, Jones BD. Extrapyramidal Symptom Rating Scale. Can J Neurol Sci. 1980;7:233.
-
- Citrome L. Olanzapine pamoate: a stick in time? A review of the efficacy and safety profile of a new depot formulation of a second-generation antipsychotic. Int J Clin Pract. 2009;63:140–150. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
