

Functional assessment of coronary artery flow using adenosine stress dual-energy CT: a preliminary study
- PMID: 20686853
- PMCID: PMC3092061
- DOI: 10.1007/s10554-010-9676-2
Functional assessment of coronary artery flow using adenosine stress dual-energy CT: a preliminary study
Abstract
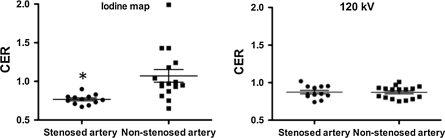
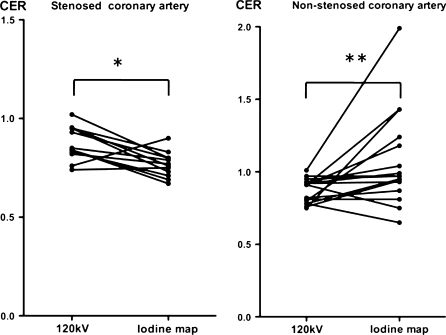
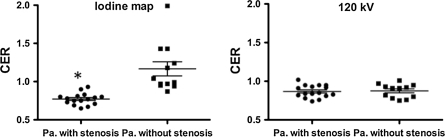
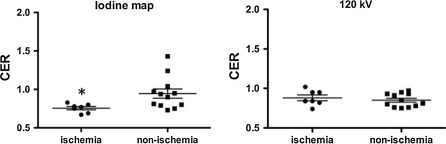
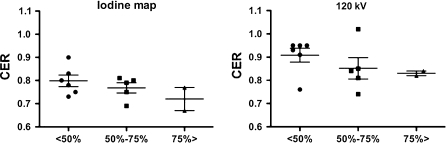
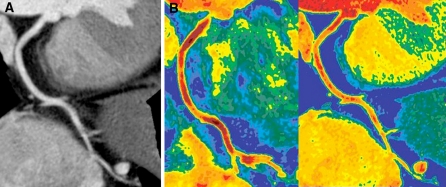
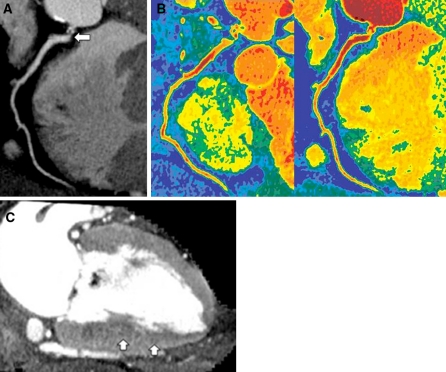
We attempted to assess coronary artery flow using adenosine-stress and dual-energy mode with dual-source CT (DE-CT). Data of 18 patients with suspected coronary arteries disease who had undergone cardiac DE-CT were retrospectively analyzed. The patients were divided into two groups: 10 patients who performed adenosine stress CT, and 8 patients who performed rest CT as controls. We reconstructed an iodine map and composite images at 120 kV (120 kV images) using raw data with scan parameters of 100 and 140 kV. We measured mean attenuation in the coronary artery proximal to the distal portion on both the iodine map and 120 kV images. Coronary enhancement ratio (CER) was calculated by dividing mean attenuation in the coronary artery by attenuation in the aortic root, and was used as an estimate of coronary enhancement. Coronary stenosis was identified as a reduction in diameter of >50% on CT angiogram, and myocardial ischemia was diagnosed by adenosine-stress myocardial perfusion scintigraphy. The iodine map showed that CER was significantly lower for ischemic territories (0.76 ± 0.06) or stenosed coronary arteries (0.77 ± 0.06) than for non-ischemic territories (0.95 ± 0.21, P=0.02) or non-stenosed coronary arteries (1.07 ± 0.33, P<0.001). The 120 kV images showed no difference in CER between these two groups. Use of CER on the iodine map separated ischemic territories from non-ischemic territories with a sensitivity of 86% and a specificity of 75%. Our quantification is the first non-invasive analytical technique for assessment of coronary artery flow using cardiac CT. CER on the iodine map is a candidate method for demonstration of alteration in coronary artery flow under adenosine stress, which is related to the physiological significance of coronary artery disease.
© The Author(s) 2010.
Figures
References
-
- Kern MJ, Lerman A, Bech JW, et al. Physiological assessment of coronary artery disease in the cardiac catheterization laboratory: a scientific statement from the American Heart Association Committee on Diagnostic and Interventional Cardiac Catheterization, Council on Clinical Cardiology. Circulation. 2006;114:1321–1341. doi: 10.1161/CIRCULATIONAHA.106.177276. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
