

Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults
- PMID: 20687087
- PMCID: PMC6465032
- DOI: 10.1002/14651858.CD007429.pub2
Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults
Abstract
Background: Dislocation of the acromioclavicular joint is one of the most common shoulder problems in general orthopaedic practice. The question of whether surgery should be used remains controversial.
Objectives: To assess the relative effects of surgical versus conservative (non-surgical) interventions for treating acromioclavicular dislocations in adults.
Search strategy: We searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (to February 2009), the Cochrane Central Register of Controlled Trials (The Cochrane Library 2009, Issue 1), MEDLINE (1966 to February 2009), EMBASE (1988 to February 2009), and LILACS (1982 to February 2009), trial registries and reference lists of articles. There were no restrictions based on language or publication status.
Selection criteria: All randomised and quasi-randomised trials that compared surgical with conservative treatment of acromioclavicular dislocation in adults were included.
Data collection and analysis: All review authors independently performed study selection. Two authors independently assessed the included trials and performed data extraction.
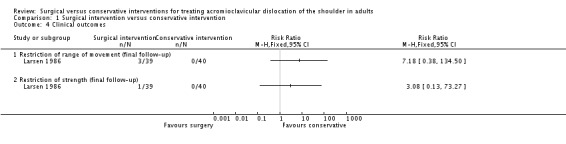
Main results: Three trials were included in this review. These involved a total of 174 mainly male participants. Two trials were randomised and one was quasi-randomised. None used validated measures for assessing functional outcome.Fixation of the acromioclavicular joint using coracoclavicular screws, acromioclavicular pins or, usually threaded, wires was compared with supporting the arm in a sling or similar device. There were no significant differences between the two groups in unsatisfactory longer-term (one year) shoulder function based on a composite measure including pain, movement and strength or function (risk ratio 1.49, 95% confidence interval 0.75 to 2.95), nor in treatment failure that generally required an operation (risk ratio 1.72, 95% confidence interval 0.72 to 4.12). However, there were fixation failures in all three trials. Particularly, the trial using wires reported a high incidence of wire breakage (16/39 (41%)). Two trials reported that surgery significantly delayed the return to work. The methods used in the three trials also meant a routine second operation for implant removal was necessary.
Authors' conclusions: There is insufficient evidence from randomised controlled trials to determine when surgical treatment is indicated for acromioclavicular dislocation in adults in current practice. Sufficiently powered, good quality, well-reported randomised trials of currently-used surgical interventions versus conservative treatment for well-defined injuries are required.
Conflict of interest statement
None known.
Figures








Update of
- doi: 10.1002/14651858.CD007429
References
References to studies included in this review
-
- Bannister GC, Wallace WA, Stableforth PG, Hutson MA. The management of acute acromioclavicular dislocation. A randomised prospective controlled trial. Journal of Bone & Joint Surgery ‐ British Volume 1989;71(5):848‐50. [MEDLINE: ] - PubMed
-
- Imatani RJ, Hanlon JJ, Cady GW. Acute, complete acromioclavicular separation. Journal of Bone & Joint Surgery ‐ American Volume 1975;57(3):328‐32. [MEDLINE: ] - PubMed
-
- Larsen E, Bjerg‐Nielsen A, Christensen P. Conservative or surgical treatment of acromioclavicular dislocation. A prospective, controlled, randomized study. Journal of Bone & Joint Surgery ‐ American Volume 1986;68(4):552‐5. [MEDLINE: ] - PubMed
References to studies excluded from this review
-
- Galpin RD, Hawkins RJ, Grainger RW. A comparative analysis of operative versus nonoperative treatment of Grade III acromioclavicular separations. Clinical Orthopaedics & Related Research 1985;(193):150‐5. - PubMed
-
- Sehmisch S, Stürmer EK, Zabka K, Losch A, Brunner U, Stürmer KM, et al. Results of a prospective multicenter trial for treatment of acromioclavicular dislocation [Ergebnisse einer prospektiven Multicenterstudie zur Behandlung der Schultereckgelenksprengung]. Sportverletz Sportschaden 2008;22(3):139‐45. [MEDLINE: ] - PubMed
-
- Sternick MB, Farias Filho OC, Carvalho MI. Acromioclavicular dislocation: prospective study [Luxaçäo acromioclavicular: estudo prospectivo]. Revista Brasileira de Ortopedia 1991;26(9):308‐12.
References to ongoing studies
-
- Joukainen A. A prospective, randomised long‐term follow‐up of operative versus non‐operative treatment of Gr. 3 acromioclavicular dislocation. clinicaltrials.gov/ct2/show/NCT00840593 (accessed 24 November 2009). [: ClinicalTrials.gov ID: NCT00840593]
-
- McKee MD, Schemitsch EH. Non‐operative versus operative treatment of acute acromioclavicular joint dislocation (ACJoint). clinicaltrials.gov/ct2/show/NCT00594841 (accessed 24 November 2009). [: ClinicalTrials.gov ID: NCT00594841]
Additional references
-
- Allman FL Jr. Fractures and ligamentous injuries of the clavicle and its articulation. Journal of Bone & Joint Surgery ‐ American Volume 1967;49(4):774‐84. - PubMed
-
- Bannister GC, Wallace WA, Stableforth PG, Hutson MA. The management of acute acromioclavicular dislocation. A randomised prospective controlled trial. Journal of Bone & Joint Surgery ‐ British Volume 1989;71(5):848‐50. - PubMed
-
- Bishop JY, Kaeding C. Treatment of the acute traumatic acromioclavicular separation. Sports Medicine & Arthroscopy Review 2006;14(4):237‐45. - PubMed
-
- Bowers RF. Complete acromioclavicular separation: Diagnoses and operative treatment. Journal of Bone & Joint Surgery ‐ American Volume 1935;17(4):1005‐10.
-
- Bäthis H, Tingart M, Bouillon B, Tiling T. Conservative or surgical therapy of acromioclavicular joint injury‐‐what is reliable? A systematic analysis of the literature using "evidence‐based medicine" criteria [Konservative oder operative Therapie der Schultereckgelenkverletzung – was ist gesichert ? Eine systematische Literaturanalyse nach Kriterien der "evidence based medicine"]. Der Chirurg 2000;71(9):1082‐9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical