

Intersubject variability of foveal cone photoreceptor density in relation to eye length
- PMID: 20688730
- PMCID: PMC3055782
- DOI: 10.1167/iovs.10-5499
Intersubject variability of foveal cone photoreceptor density in relation to eye length
Abstract
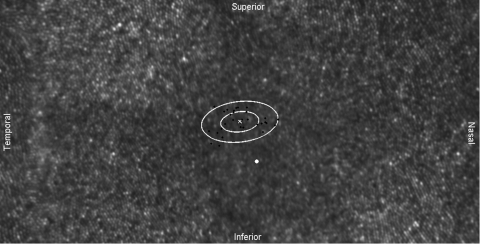
Purpose: Adaptive optics scanning laser ophthalmoscopy (AOSLO) under optimized wavefront correction allows for routine imaging of foveal cone photoreceptors. The intersubject variability of foveal cone density was measured and its relation to eye length evaluated.
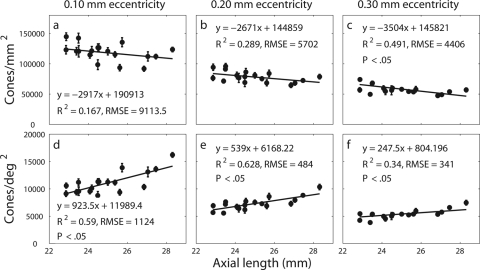
Methods: AOSLO was used to image 18 healthy eyes with axial lengths from 22.86 to 28.31 mm. Ocular biometry and an eye model were used to estimate the retinal magnification factor. Individual cones in the AOSLO images were labeled, and the locations were used to generate topographic maps representing the spatial distribution of density. Representative retinal (cones/mm(2)) and angular (cones/deg(2)) cone densities at specific eccentricities were calculated from these maps.
Results: The entire foveal cone mosaic was resolved in four eyes, whereas the cones within 0.03 mm eccentricity remained unresolved in most eyes. The preferred retinal locus deviated significantly (P < 0.001) from the point of peak cone density for all except one individual. A significant decrease in retinal density (P < 0.05) with increasing axial length was observed at 0.30 mm eccentricity but not closer. Longer, more myopic eyes generally had higher angular density near the foveal center than the shorter eyes, but by 1°, this difference was nullified by retinal expansion, and so angular densities across all eyes were similar.
Conclusions: The AOSLO can resolve the smallest foveal cones in certain eyes. Although myopia causes retinal stretching in the fovea, its effect within the foveola is confounded by factors other than cone density that have high levels of intersubject variability.
Figures







References
-
- Chui TYP, Yap MKH, Chan HHL, Thibos LN. Retinal stretching limits peripheral visual acuity in myopia. Vision Res. 2005;45:593–605 - PubMed
-
- Coletta NJ, Watson T. Effect of myopia on visual acuity measured with laser interference fringes. Vision Res. 2006;46:636–651 - PubMed
-
- Strang NC, Winn B, Bradley A. The role of neural and optical factors in limiting visual resolution in myopia. Vision Res. 1998;38:1713–1721 - PubMed
-
- Bullimore MA, Gilmartin B, Royston JM. Steady-state accommodation and ocular biometry in late-onset myopia. Doc Ophthalmol. 1992;80:143–155 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
