

Improved regulatory T-cell activity in patients with chronic immune thrombocytopenia treated with thrombopoietic agents
- PMID: 20688957
- PMCID: PMC2996119
- DOI: 10.1182/blood-2010-04-281717
Improved regulatory T-cell activity in patients with chronic immune thrombocytopenia treated with thrombopoietic agents
Abstract
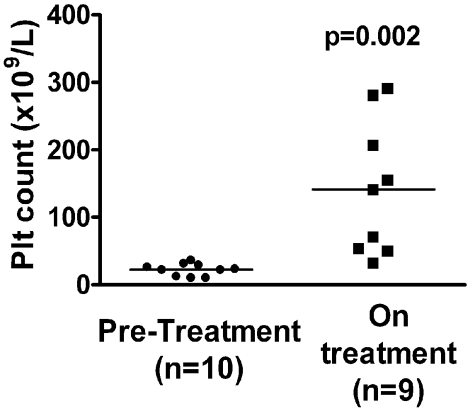
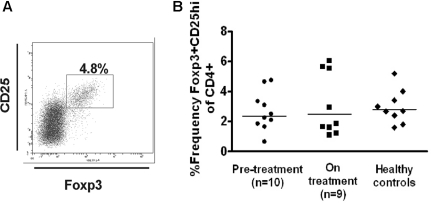
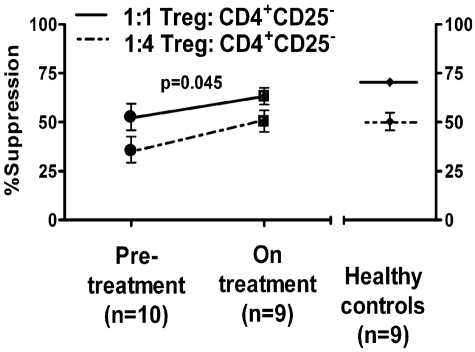
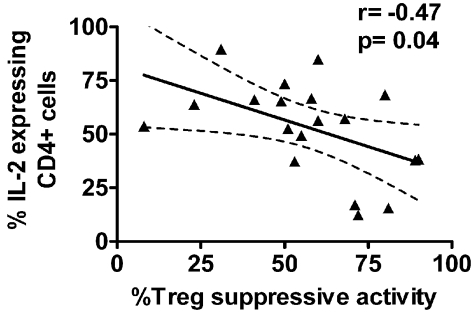
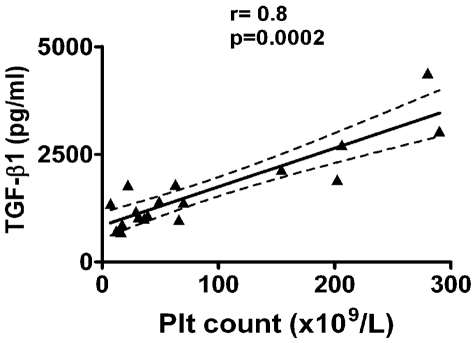
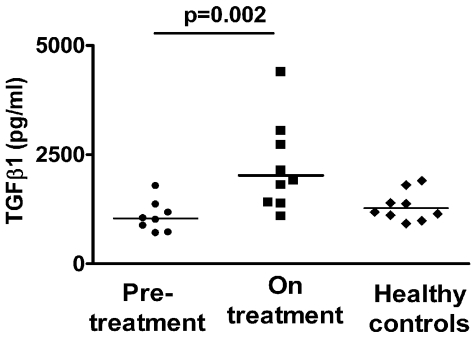
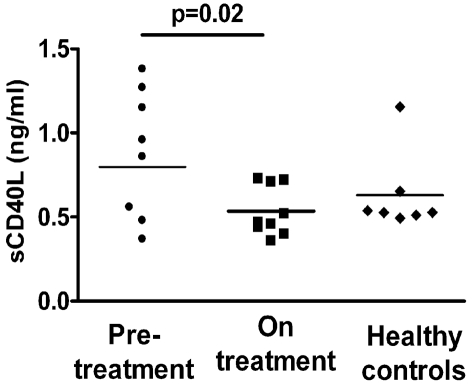
Immune thrombocytopenia (ITP) is an autoantibody-mediated bleeding disorder with both accelerated platelet destruction and impaired platelet production. We and others have described impaired regulatory CD4(+)CD25(hi) T cells (Treg) numbers and/or suppressive function in ITP patients. Clinical trials using thrombopoietic agents to stimulate platelet production have shown favorable outcomes in ITP patients, but information on the immunologic responses of treated patients are lacking. We studied the immunologic profile of chronic ITP patients before (n = 10) and during treatment with thrombopoietin receptor (TPO-R) agonists (n = 9). Treg activity, as measured by suppression of proliferation of autologous CD4(+) CD25(-) cells, was improved in patients on treatment (P < .05), and the improvement correlated with reduction in interleukin-2-producing CD4(+) cells, consistent with dampening of immune responses. There was a concomitant increase in total circulating transforming growth factor-β1 (TGF-β1) levels (P = .002) in patients on treatment, and the levels of TGF-β1 correlated with the degree of improvement in platelet counts (r = .8, P = .0002). This suggests that platelets in patients on TPO-R treatment may play a role in improving Treg function, either directly or indirectly by enhanced release of TGF-β1 as a result of greater platelet turnover. In conclusion, our findings suggest that thrombopoietic agents in patients with ITP have profound effects to restore immune tolerance.
Figures
Comment in
-
ITP: Tregs come to the rescue.Blood. 2010 Nov 25;116(22):4388-90. doi: 10.1182/blood-2010-09-302364. Blood. 2010. PMID: 21109623 No abstract available.
Similar articles
-
Functional role of CD4+CD25+ regulatory T cells and transforming growth factor-beta1 in childhood immune thrombocytopenic purpura.Egypt J Immunol. 2006;13(1):173-87. Egypt J Immunol. 2006. PMID: 17974160
-
The pathophysiology of ITP revisited: ineffective thrombopoiesis and the emerging role of thrombopoietin receptor agonists in the management of chronic immune thrombocytopenic purpura.Hematology Am Soc Hematol Educ Program. 2008:219-26. doi: 10.1182/asheducation-2008.1.219. Hematology Am Soc Hematol Educ Program. 2008. PMID: 19074086
-
CD4+CD25+Foxp3+ regulatory T cells in the pathophysiology of immune thrombocytopenia.Semin Hematol. 2013 Jan;50 Suppl 1:S43-9. doi: 10.1053/j.seminhematol.2013.03.018. Semin Hematol. 2013. PMID: 23664516 Review.
-
The cytokines (IFN-gamma, IL-2, IL-4, IL-10, IL-17) and Treg cytokine (TGF-beta1) levels in adults with immune thrombocytopenia.Pharmazie. 2014 Sep;69(9):694-7. Pharmazie. 2014. PMID: 25272942
-
Application of thrombopoietic agents in cancer therapy-induced thrombocytopenia: A comprehensive review.Blood Rev. 2025 Mar;70:101257. doi: 10.1016/j.blre.2025.101257. Epub 2025 Jan 11. Blood Rev. 2025. PMID: 39809679 Review.
Cited by
-
Eltrombopag-based combination treatment for immune thrombocytopenia.Ther Adv Hematol. 2018 Oct 4;9(10):309-317. doi: 10.1177/2040620718798798. eCollection 2018 Oct. Ther Adv Hematol. 2018. PMID: 30344993 Free PMC article. Review.
-
Platelet and peripheral white blood cell counts at diagnosis predict the response of adult immune thrombocytopenia to recombinant human interleukin-11: A retrospective, single-center, case-control study.Medicine (Baltimore). 2019 Apr;98(16):e15195. doi: 10.1097/MD.0000000000015195. Medicine (Baltimore). 2019. PMID: 31008943 Free PMC article.
-
Pathogenesis of refractory ITP: Overview.Br J Haematol. 2023 Oct;203(1):10-16. doi: 10.1111/bjh.19083. Br J Haematol. 2023. PMID: 37735546 Free PMC article. Review.
-
Emerging Concepts in Immune Thrombocytopenia.Front Immunol. 2018 Apr 30;9:880. doi: 10.3389/fimmu.2018.00880. eCollection 2018. Front Immunol. 2018. PMID: 29760702 Free PMC article. Review.
-
Clinical spectrum, outcome and management of immune thrombocytopenia associated with myelodysplastic syndromes and chronic myelomonocytic leukemia.Haematologica. 2021 May 1;106(5):1414-1422. doi: 10.3324/haematol.2020.272559. Haematologica. 2021. PMID: 33626866 Free PMC article.
References
-
- Cohen YC, Djulbegovic B, Shamai-Lubovitz O, Mozes B. The bleeding risk and natural history of idiopathic thrombocytopenic purpura in patients with persistent low platelet counts. Arch Intern Med. 2000;160(11):1630–1638. - PubMed
-
- Michel M. Immune thrombocytopenic purpura: epidemiology and implications for patients. Eur J Haematol Suppl. 2009;71:3–7. - PubMed
-
- Gernsheimer T. Chronic idiopathic thrombocytopenic purpura: mechanisms of pathogenesis. Oncologist. 2009;14(1):12–21. - PubMed
-
- Filion MC, Proulx C, Bradley AJ, et al. Presence in peripheral blood of healthy individuals of autoreactive T cells to a membrane antigen present on bone marrow-derived cells. Blood. 1996;88(6):2144–2150. - PubMed
-
- Semple JW, Freedman J. Increased antiplatelet T helper lymphocyte reactivity in patients with autoimmune thrombocytopenia. Blood. 1991;78(10):2619–2625. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
