

Pathogenic role of Demodex mites in blepharitis
- PMID: 20689407
- PMCID: PMC2946818
- DOI: 10.1097/ACI.0b013e32833df9f4
Pathogenic role of Demodex mites in blepharitis
Abstract
Purpose of review: To summarize the key literature and our research experience regarding Demodex infestation as a potential cause of ocular inflammatory diseases with a special emphasis on Demodex blepharitis.
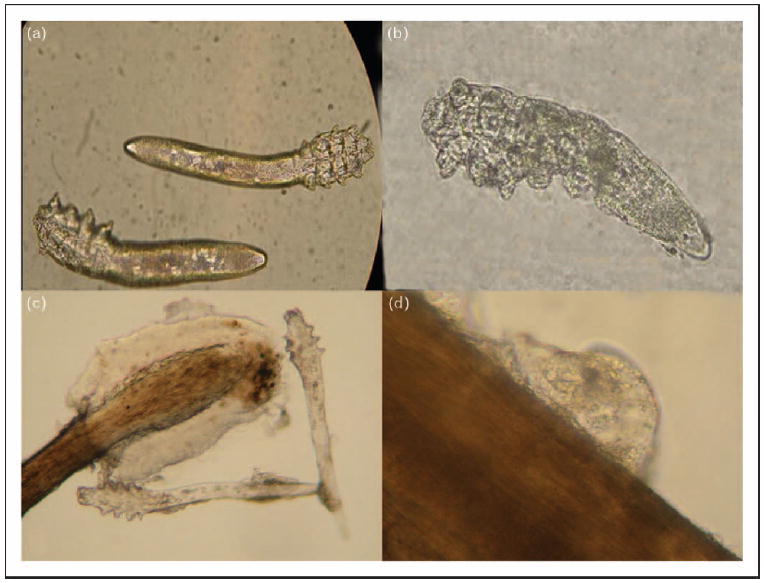
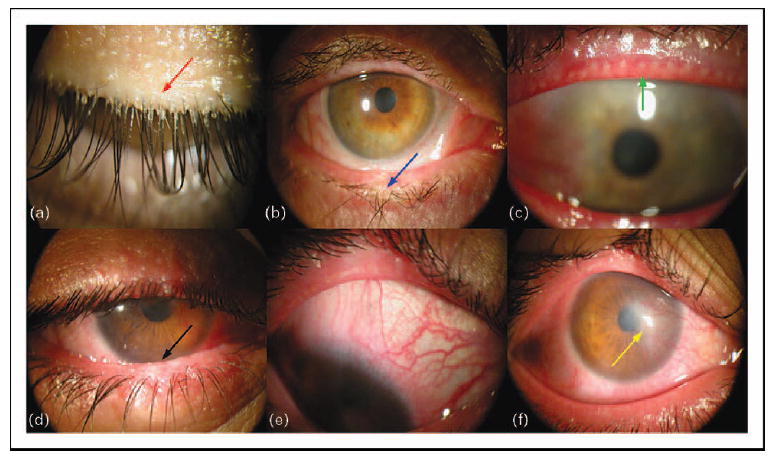
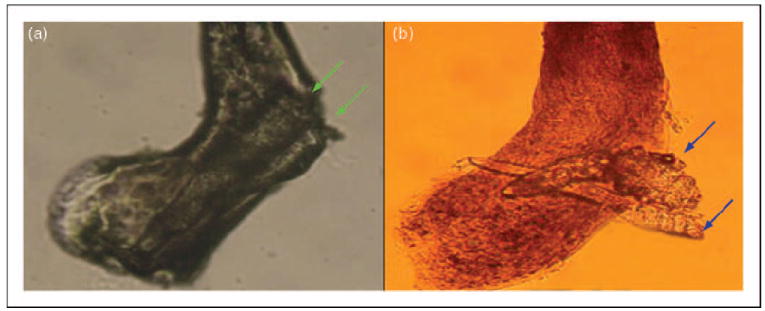
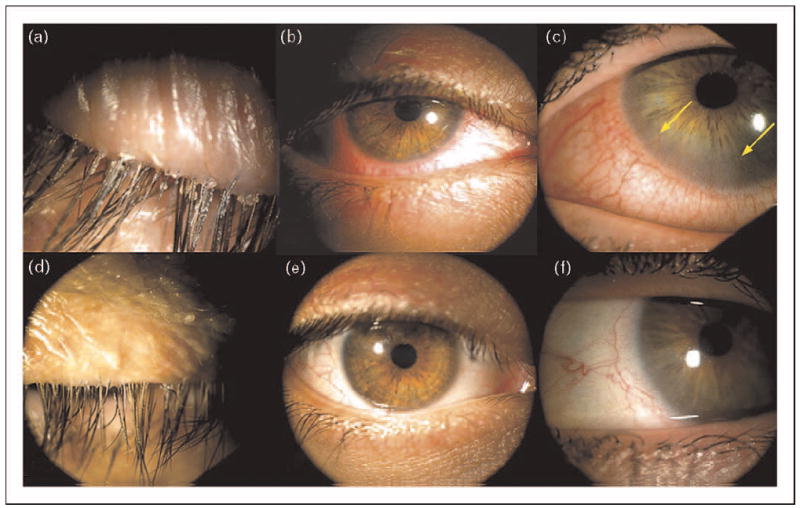
Recent findings: Two distinct Demodex species have been confirmed as a cause of blepharitis: Demodex folliculorum can cause anterior blepharitis associated with disorders of eyelashes, and D. brevis can cause posterior blepharitis with meibomian gland dysfunction and keratoconjunctivitis. Tea tree oil treatments with either 50% lid scrubs or 5% lid massages are effective in eradicating mites and reducing ocular surface inflammation.
Summary: Demodex blepharitis is a common but overlooked external eye disease. The pathogenesis of Demodex blepharitis in eliciting ocular surface inflammation has been further clarified. The modified eyelash sampling and counting method makes it easier and more accurate to diagnose Demodex infestation. Tea tree oil shows promising potential to treat Demodex blepharitis by reducing Demodex counts with additional antibacterial, antifungal, and anti-inflammatory actions.
Figures
References
-
- Post CF, Juhlin E. Demodex folliculorum and blepharitis. Arch Dermatol. 1963;88:298–302. - PubMed
-
- Basta-Juzbasic A, Subic JS, Ljubojevic S. Demodex folliculorum in development of dermatitis rosaceiformis steroidica and rosacea-related diseases. Clin Dermatol. 2002;20:135–140. - PubMed
-
- Erbagci Z, Ozgoztasi O. The significance of Demodex folliculorum density in rosacea. Int J Dermatol. 1998;37:421–425. - PubMed
-
- Forton F, Germaux MA, Brasseur T, et al. Demodicosis and rosacea: epidemiology and significance in daily dermatologic practice. J Am Acad Dermatol. 2005;52:74–87. - PubMed
-
- Georgala S, Katoulis AC, Kylafis GD, et al. Increased density of Demodex folliculorum and evidence of delayed hypersensitivity reaction in subjects with papulopustular rosacea. J Eur Acad Dermatol Venereol. 2001;15:441–444. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
