

Endoscopic Ultrasound-Guided Fine Needle Aspiration (EUS-FNA) Diagnosis of Recurrent Anal Cancer After Chemoradiation and Negative Forceps Biopsies: A Case Report
- PMID: 20689610
- PMCID: PMC2872600
- DOI: 10.4137/cmo.s993
Endoscopic Ultrasound-Guided Fine Needle Aspiration (EUS-FNA) Diagnosis of Recurrent Anal Cancer After Chemoradiation and Negative Forceps Biopsies: A Case Report
Abstract
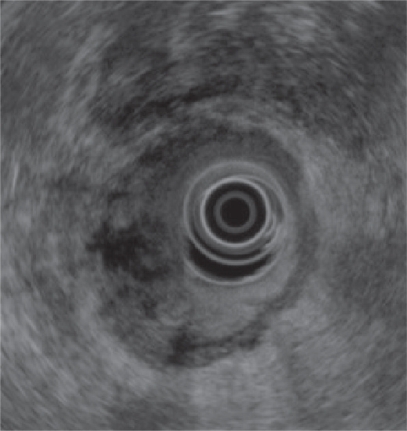
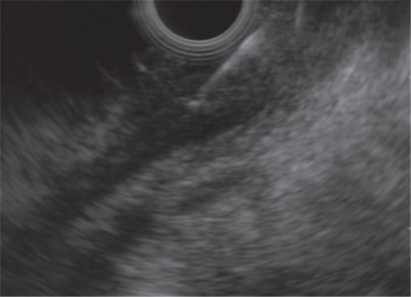
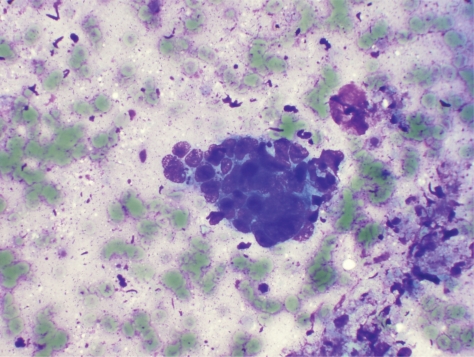
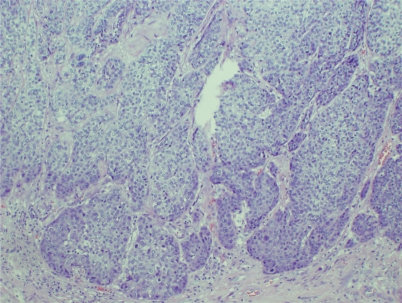
A 69-year-old woman with a history of uT2 N0 post-treated anal squamous cell cancer (SCC) presented for EUS for perianal pain. Two months prior, a digital rectal examination was significant for an indurated lesion on the left lateral rectal wall just proximal to the dentate line. A sigmoidoscopy revealed mild narrowing of the anal canal and an ulcerated friable mucosa in the same area. A biopsy demonstrated ulceration without malignancy. EUS showed a hypoechoic, non-circumferential, left-sided distal rectal mass. EUS-FNA was performed. Cytology demonstrated poorly differentiated SCC. This was confirmed by subsequent surgical resection. While endoscopic biopsy of suspected anal recurrences is usually sufficient, histologic or cytologic confirmation are necessary, as radiation-induced changes are difficult to differentiate from tumor recurrence. This case demonstrates that EUS-FNA is useful in surveillance of anal SCC when there is a high clinical suspicion of recurrence.
Figures

Similar articles
-
Needle tract seeding following endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a report of two cases.World J Surg Oncol. 2019 Aug 5;17(1):134. doi: 10.1186/s12957-019-1681-x. World J Surg Oncol. 2019. PMID: 31382964 Free PMC article.
-
Endoscopic ultrasound-guided fine needle aspiration as a diagnostic and staging tool for rectal and perirectal lesions-an institutional experience.Ann Diagn Pathol. 2013 Dec;17(6):494-7. doi: 10.1016/j.anndiagpath.2013.08.002. Epub 2013 Sep 9. Ann Diagn Pathol. 2013. PMID: 24028888
-
Pretherapeutic evaluation of patients with upper gastrointestinal tract cancer using endoscopic and laparoscopic ultrasonography.Dan Med J. 2012 Dec;59(12):B4568. Dan Med J. 2012. PMID: 23290296 Review.
-
Endoscopic ultrasound-guided fine-needle aspiration in 179 cases: the M. D. Anderson Cancer Center experience.Cancer. 2002 Jun 25;96(3):174-80. doi: 10.1002/cncr.10614. Cancer. 2002. PMID: 12115306
-
Needle tract seeding recurrence of pancreatic cancer in the gastric wall with paragastric lymph node metastasis after endoscopic ultrasound-guided fine needle aspiration followed by pancreatectomy: a case report and literature review.BMC Gastroenterol. 2020 Jan 15;20(1):13. doi: 10.1186/s12876-020-1159-x. BMC Gastroenterol. 2020. PMID: 31941458 Free PMC article. Review.
Cited by
-
Rectal Endoscopic Ultrasound in Clinical Practice.Curr Gastroenterol Rep. 2019 Apr 12;21(4):18. doi: 10.1007/s11894-019-0682-9. Curr Gastroenterol Rep. 2019. PMID: 30980194 Review.
-
Practical approach to linear endoscopic ultrasound examination of the rectum and anal canal.Endosc Int Open. 2022 Oct 17;10(10):E1417-E1426. doi: 10.1055/a-1922-6500. eCollection 2022 Oct. Endosc Int Open. 2022. PMID: 36262505 Free PMC article. Review.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA: a cancer journal for clinicians. 2006;56:106–30. - PubMed
-
- Mackay SG, Pager CK, Joseph D, et al. Assessment of the accuracy of transrectal ultrasonography in anorectal neoplasia. The British Journal of Surgery. 2003;90:346–50. - PubMed
-
- Tarantino D, Bernstein MA. Endoanal ultrasound in the staging and management of squamous-cell carcinoma of the anal canal: potential implications of a new ultrasound staging system. Diseases of the Colon and Rectum. 2002;45:16–22. - PubMed
-
- Babb RR. Radiation proctitis: a review. Am J Gastroenterol. 1996;91:1309–11. - PubMed
-
- Eng C. Anal cancer: current and future methodology. Cancer Investigation. 2006;24:535–44. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
