

Surgical approaches to epicardial pacemaker placement: does pocket location affect lead survival?
- PMID: 20690018
- PMCID: PMC2948166
- DOI: 10.1007/s00246-010-9754-1
Surgical approaches to epicardial pacemaker placement: does pocket location affect lead survival?
Abstract
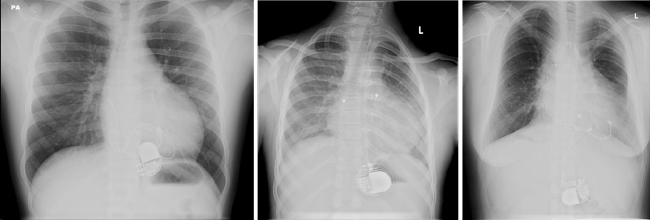
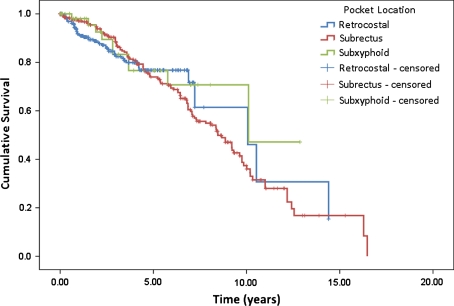
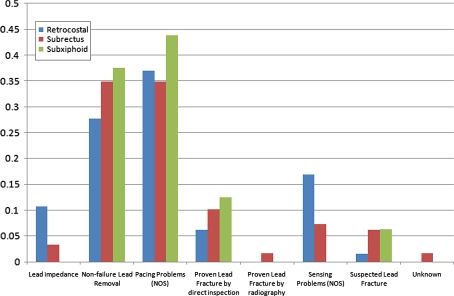
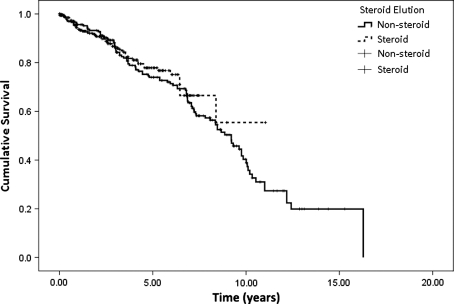
Permanent cardiac pacing in pediatric patients presents challenges related to small patient size, complex anatomy, electrophysiologic abnormalities, and limited access to cardiac chambers. Epicardial pacing currently remains the conventional technique for infants and patients with complex congenital heart disease. Pacemaker lead failure is the major source of failure for such epicardial systems. The authors hypothesized that a retrocostal surgical approach would reduce the rate of lead failure due to fracture compared with the more traditional subrectus and subxiphoid approaches. To evaluate this hypothesis, a retrospective chart review analyzed patients with epicardial pacemaker systems implanted or followed at Rady Children's Hospital San Diego between January 1980 and May 2007. The study cohort consisted of 219 patients and a total of 620 leads with epicardial pacemakers. Among these patients, 84% had structural congenital heart disease, and 45% were younger than 3 years at time of the first implantation. The estimated lead survival was 93% at 2 years and 83% at 5 years. The majority of leads failed due to pacing problems (54%), followed by lead fracture (31%) and sensing problems (14%). When lead failure was adjusted for length of follow-up period, no significant differences in the rates of failure by pocket location were found.
Figures
Similar articles
-
Performance of steroid eluting bipolar epicardial leads in pediatric and congenital heart disease patients: 15 years of single center experience.J Cardiothorac Surg. 2014 May 12;9:84. doi: 10.1186/1749-8090-9-84. J Cardiothorac Surg. 2014. PMID: 24886320 Free PMC article.
-
Long-term atrial and ventricular epicardial pacemaker lead survival after cardiac operations in pediatric patients with congenital heart disease.Heart Rhythm. 2015 Mar;12(3):566-573. doi: 10.1016/j.hrthm.2014.12.001. Epub 2014 Dec 4. Heart Rhythm. 2015. PMID: 25484105
-
Efficacy of prophylactic epicardial pacing leads in children and young adults.Ann Thorac Surg. 2004 Jul;78(1):197-202; discussion 202-3. doi: 10.1016/j.athoracsur.2004.02.008. Ann Thorac Surg. 2004. PMID: 15223427 Review.
-
Patient, procedural, and hardware factors associated with pacemaker lead failures in pediatrics and congenital heart disease.Heart Rhythm. 2004 Jul;1(2):150-9. doi: 10.1016/j.hrthm.2004.02.020. Heart Rhythm. 2004. PMID: 15851146
-
How pacemakers work and simple programming: a primer for the non-electrophysiologist.Cardiol Young. 2017 Jan;27(S1):S115-S120. doi: 10.1017/S1047951116002341. Cardiol Young. 2017. PMID: 28084968 Review.
Cited by
-
Performance of steroid eluting bipolar epicardial leads in pediatric and congenital heart disease patients: 15 years of single center experience.J Cardiothorac Surg. 2014 May 12;9:84. doi: 10.1186/1749-8090-9-84. J Cardiothorac Surg. 2014. PMID: 24886320 Free PMC article.
-
Minimally Invasive Epicardial Pacemaker Implantation in Neonates with Congenital Heart Block.Arq Bras Cardiol. 2017 Oct;109(4):331-339. doi: 10.5935/abc.20170126. Epub 2017 Sep 4. Arq Bras Cardiol. 2017. PMID: 28876373 Free PMC article.
-
Ischemic Heart Disease with In-Stent Re-Stenosis with Complete Heart Block and Isolated Persistent Left Superior Vena Cava - Rare Case Report with Challenges and Clinical Implications.Ann Card Anaesth. 2024 Jul 1;27(3):270-273. doi: 10.4103/aca.aca_166_23. Epub 2024 Jul 4. Ann Card Anaesth. 2024. PMID: 38963367 Free PMC article.
-
Intraoperative localization of cardiac conduction tissue regions using real-time fibre-optic confocal microscopy: first in human trial.Eur J Cardiothorac Surg. 2020 Aug 1;58(2):261-268. doi: 10.1093/ejcts/ezaa040. Eur J Cardiothorac Surg. 2020. PMID: 32083653 Free PMC article.
-
Old but not forgotten: Creative use of abandoned epicardial leads after more than 2 decades.HeartRhythm Case Rep. 2017 Oct 19;3(12):559-561. doi: 10.1016/j.hrcr.2017.05.006. eCollection 2017 Dec. HeartRhythm Case Rep. 2017. PMID: 29296574 Free PMC article. No abstract available.
References
-
- Cutler NG, Karpawich PP, Cavitt D, Hakimi M, Walter HL. Steroid-eluting epicardial pacing electrodes: six-year experience of pacing thresholds in a growing pediatric population. Pace. 1997;20:2943–2948. - PubMed
-
- Dodge-Khatami A, Kadner A, Dave H, Rahn M, Prêtre R, Bauersfeld U. Left heart atrial and ventricular epicardial pacing through a left lateral thoracotomy in children: a safe approach with excellent functional and cosmetic results. Eur J Cardiothorac Surg. 2005;28:541–545. doi: 10.1016/j.ejcts.2005.06.040. - DOI - PubMed
-
- Epstein MR, Walsh EP, Saul JP, Triedman JK, Mayer JE, Gamble WJ. Long-term performance of bipolar epicardial atrial pacing using an active fixation bipolar endocardial lead. Pace. 1998;21:1098–1104. - PubMed
