

Effect of price increase of adrenocorticotropic hormone on treatment practices of infantile spasms
- PMID: 20691936
- PMCID: PMC3197710
- DOI: 10.1016/j.pediatrneurol.2010.04.005
Effect of price increase of adrenocorticotropic hormone on treatment practices of infantile spasms
Abstract
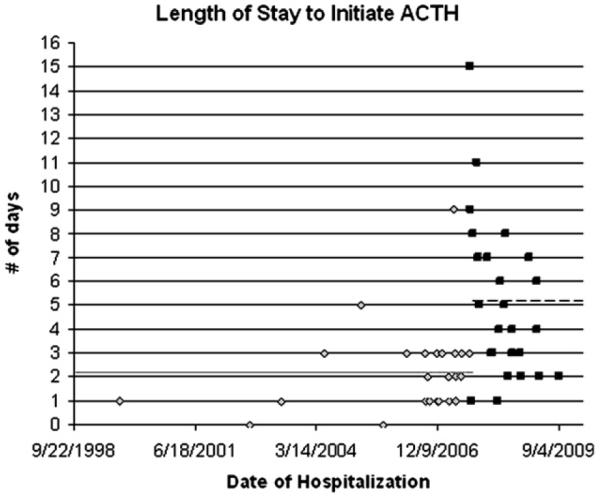
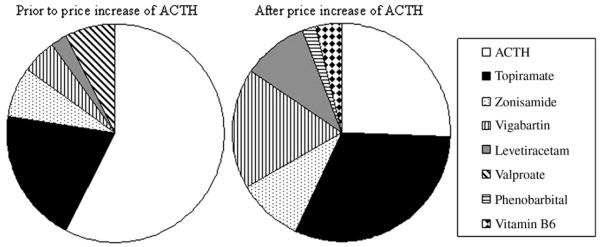
Intramuscular adrenocorticotropic hormone putatively constitutes the most efficacious treatment for infantile spasms. Adrenocorticotropic hormone in the United States is an "orphan drug," made by a single manufacturer. The price of adrenocorticotropic hormone increased almost 14-fold on August 27, 2007. We sought to evaluate the impact of this price increase on treatment practices at our institution, using a retrospective chart review of all children with infantile spasms treated during 2007-2009. We identified 97 patients whose spasms were treated using antiepileptic drugs, and we determined the length of stay for those hospitalized to initiate adrenocorticotropic hormone. Patients before the price increase were more likely to have been treated with adrenocorticotropic hormone as first medication, and were hospitalized 2.2 +/- 0.5 S.D. days for initiation. Patients after the price increase were more likely to have been treated initially with oral antiepileptic drugs rather than adrenocorticotropic hormone (P < 0.002). Those commencing adrenocorticotropic hormone after the price increase were hospitalized significantly longer (5.1 +/- 0.6 days S.D., P < 0.001). Treatment choices need to be evidence-based, but other factors often influence them.
Copyright 2010 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The response to ACTH is determined early in the treatment of infantile spasms.Epileptic Disord. 2015 Mar;17(1):52-7. doi: 10.1684/epd.2014.0723. Epileptic Disord. 2015. PMID: 25644547
-
Outcomes in treatment of infantile spasms with pulse methylprednisolone.J Child Neurol. 2010 Aug;25(8):948-53. doi: 10.1177/0883073809356107. Epub 2010 Feb 8. J Child Neurol. 2010. PMID: 20142465 Clinical Trial.
-
Cost-effectiveness of adrenocorticotropic hormone versus oral steroids for infantile spasms.Epilepsia. 2021 Feb;62(2):347-357. doi: 10.1111/epi.16799. Epub 2021 Jan 8. Epilepsia. 2021. PMID: 33417252
-
Major adverse events associated with treatment of infantile spasms.J Child Neurol. 2007 Dec;22(12):1360-6. doi: 10.1177/0883073807310988. J Child Neurol. 2007. PMID: 18174552
-
Treatment of infantile spasms.Pediatr Neurol. 1990 May-Jun;6(3):147-50. doi: 10.1016/0887-8994(90)90054-5. Pediatr Neurol. 1990. PMID: 2163254 Review.
Cited by
-
Comparison of Efficacy and Safety of Low- Versus High-Dose Oral Prednisolone in Infantile Spasm (IS): An Open Label Randomized Controlled Trial at the Children's Hospital & Institute of Child Health, Multan, Pakistan.Cureus. 2022 Mar 14;14(3):e23164. doi: 10.7759/cureus.23164. eCollection 2022 Mar. Cureus. 2022. PMID: 35444917 Free PMC article.
-
Effectiveness of corticosteroids versus adrenocorticotropic hormone for infantile spasms: a systematic review and meta-analysis.Ann Clin Transl Neurol. 2019 Nov;6(11):2270-2281. doi: 10.1002/acn3.50922. Epub 2019 Oct 27. Ann Clin Transl Neurol. 2019. PMID: 31657133 Free PMC article.
-
An effective initial polytherapy for children with West syndrome.Neural Regen Res. 2013 Jun 15;8(17):1623-30. doi: 10.3969/j.issn.1673-5374.2013.17.011. Neural Regen Res. 2013. PMID: 25206459 Free PMC article.
-
Preclinical Screening for Treatments for Infantile Spasms in the Multiple Hit Rat Model of Infantile Spasms: An Update.Neurochem Res. 2017 Jul;42(7):1949-1961. doi: 10.1007/s11064-017-2282-0. Epub 2017 May 2. Neurochem Res. 2017. PMID: 28462453 Free PMC article.
-
Modeling epileptic spasms during infancy: Are we heading for the treatment yet?Pharmacol Ther. 2020 Aug;212:107578. doi: 10.1016/j.pharmthera.2020.107578. Epub 2020 May 15. Pharmacol Ther. 2020. PMID: 32417271 Free PMC article. Review.
References
-
- Kossoff EH. Infantile spasms. Neurologist. 2010;16:69–75. - PubMed
-
- Bobele GB, Bodensteiner JB. The treatment of infantile spasms by child neurologists. J Child Neurol. 1994;9:432–5. - PubMed
-
- Appleton RE. The treatment of infantile spasms by paediatric neurologists in the UK and Ireland. Dev Med Child Neurol. 1996;38:278–9. - PubMed
-
- Lux AL, Edwards SW, Hancock E, et al. The United Kingdom Infantile Spasms Study comparing vigabatrin with prednisolone or tetracosactide at 14 days: A multicentre, randomised controlled trial. Lancet. 2004;364:1773–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
