

Kidney function, albuminuria, and all-cause mortality in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study
- PMID: 20692752
- PMCID: PMC2963678
- DOI: 10.1053/j.ajkd.2010.05.017
Kidney function, albuminuria, and all-cause mortality in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study
Abstract
Background: Chronic kidney disease and albuminuria are associated with increased risk of all-cause mortality.
Study design: Prospective observational cohort study.
Setting & participants: 17,393 participants (mean age, 64.3 ± 9.6 years) in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) Study.
Predictor: Estimated glomerular filtration rate (eGFR), urinary albumin-creatinine ratio (ACR).
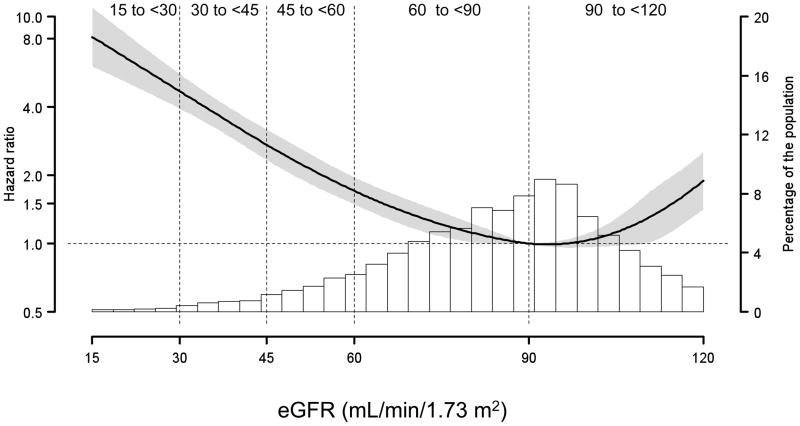
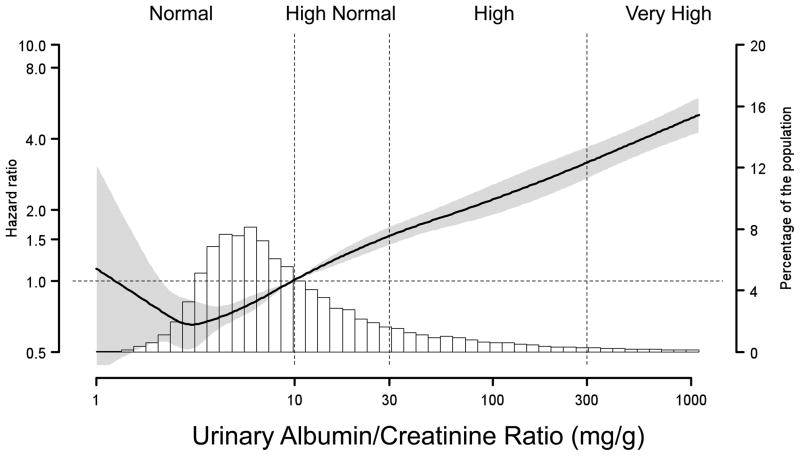
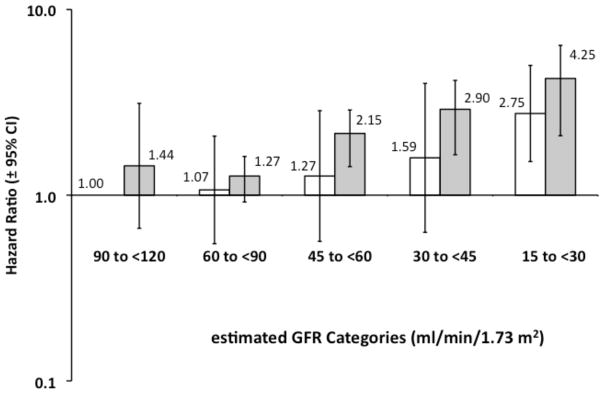
Outcome: All-cause mortality (710 deaths); median duration of follow-up, 3.6 years. MEASUREMENTS & ANALYSIS: Categories of eGFR (90 to <120, 60 to <90, 45 to <60, 30 to <45, and 15 to <30 mL/min/1.73 m(2)) and urinary ACR (<10 mg/g or normal, 10 to <30 mg/g or high normal, 30 to 300 mg/g or high, and >300 mg/g or very high). Cox proportional hazards models were adjusted for demographic factors, cardiovascular covariates, and hemoglobin level.
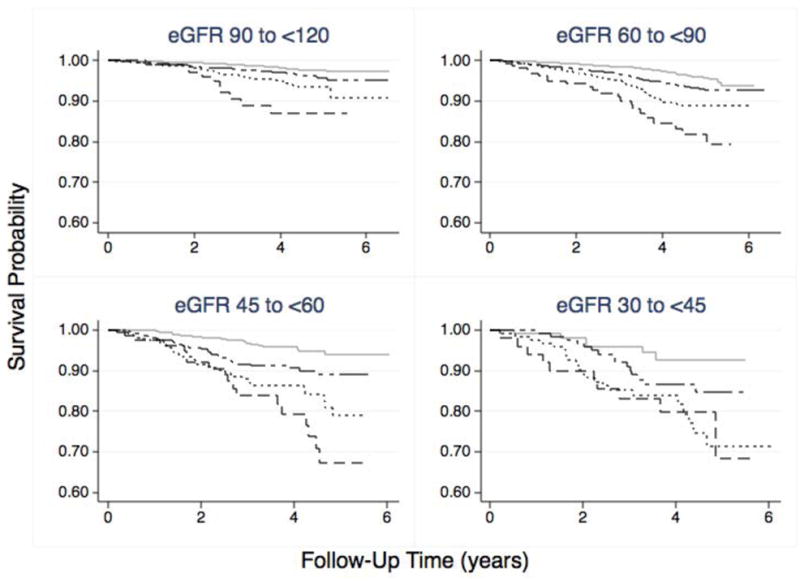
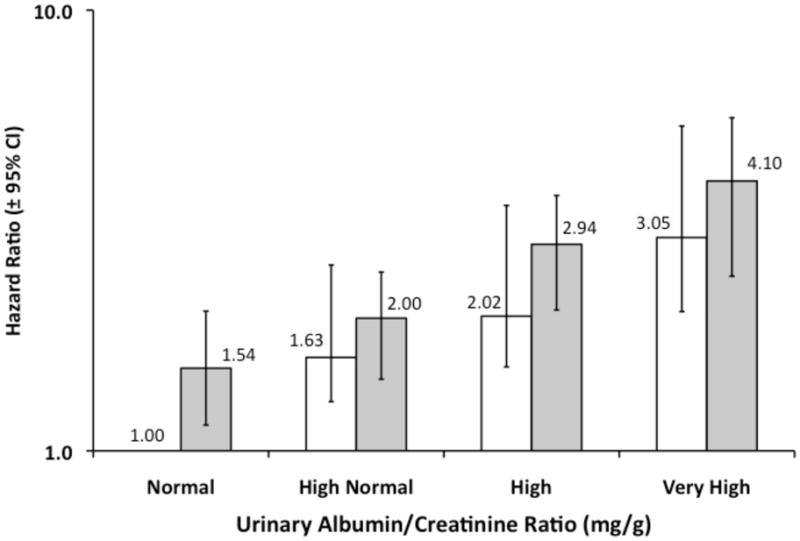
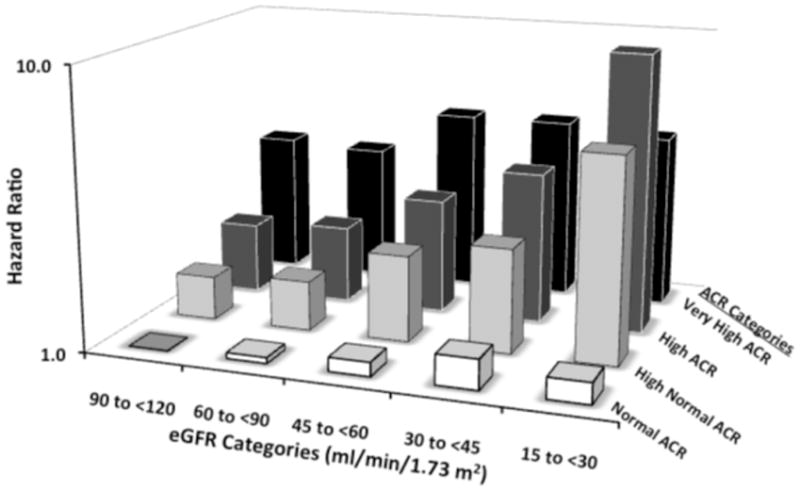
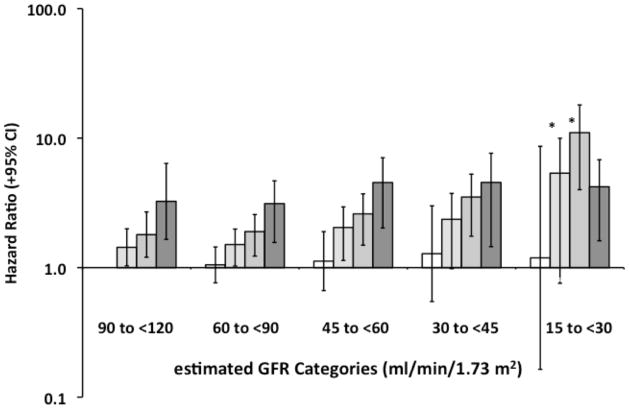
Results: The background all-cause mortality rate for participants with normal ACR, eGFR of 90 to <120 mL/min/1.73 m(2), and no coronary heart disease was 4.3 deaths/1,000 person-years. Higher ACR was associated with an increased multivariable-adjusted HR for all-cause mortality within each eGFR category. Decreased eGFR was associated with a higher adjusted HR for all-cause mortality for participants with high-normal (P = 0.01) and high (P < 0.001) ACRs, but not those with normal or very high ACRs.
Limitations: Only 1 laboratory assessment for serum creatinine and ACR was available.
Conclusions: Increased albuminuria was an independent risk factor for all-cause mortality. Decreased eGFR was associated with increased mortality risk in those with high-normal and high ACRs. The mortality rate was low in the normal-ACR group and increased in the very-high-ACR group, but did not vary with eGFR in these groups.
Copyright © 2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Levey AS, Atkins R, Coresh J, et al. Chronic kidney disease as a global public health problem: approaches and initiatives - a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007;72:247–259. - PubMed
-
- Winearls CG, Glassock RJ. Dissecting and refining the staging of chronic kidney disease. Kidney Int. 2009;75:1009–1014. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med. 2004;164:659–663. - PubMed
-
- Beattie JN, Soman SS, Sandberg KR, et al. Determinants of mortality after myocardial infarction in patients with advanced renal dysfunction. Am J Kidney Dis. 2001;37:1191–1200. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
