

Eight-year trend of acute respiratory distress syndrome: a population-based study in Olmsted County, Minnesota
- PMID: 20693377
- PMCID: PMC3040394
- DOI: 10.1164/rccm.201003-0436OC
Eight-year trend of acute respiratory distress syndrome: a population-based study in Olmsted County, Minnesota
Abstract
Rationale: significant progress has been made in understanding the pathogenesis of acute respiratory distress syndrome (ARDS). Recent advances in hospital practice may have reduced the incidence of this lethal syndrome.
Objectives: to observe incidence trends and associated outcomes of ARDS.
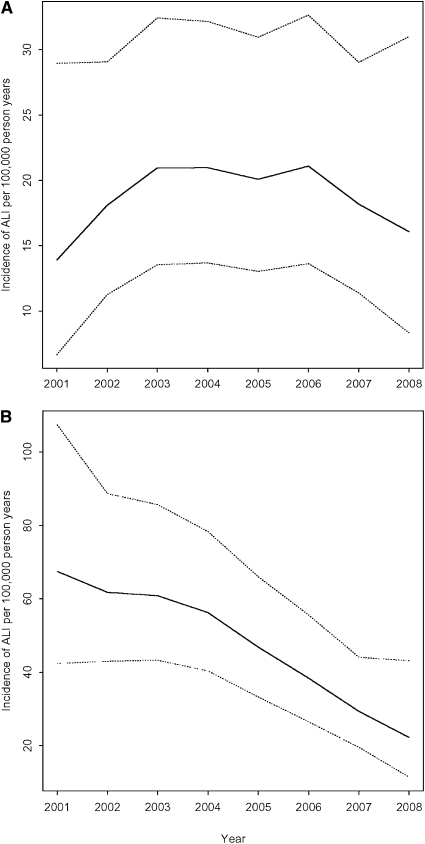
Methods: this population-based cohort study was conducted in Olmsted County, Minnesota. Using a validated screening protocol, investigators identified intensive care patients with acute hypoxemia and bilateral pulmonary infiltrates. The presence of ARDS was independently confirmed according to American-European Consensus Conference criteria. The incidence of ARDS and associated outcomes were compared over the 8-year study period (2001-2008).
Measurements and main results: over the 8-year period, critically ill Olmsted County residents presented with increasing severity of acute illness, a greater number of comorbidities, and a higher prevalence of major predisposing conditions for ARDS. The ARDS incidence decreased significantly from 82.4 to 38.9 per 100,000 person-years during the study period (P < 0.001). A decline in hospital-acquired ARDS (P < 0.001) was responsible for the fall in the incidence density with no change on admission (P = 0.877). Overall, mortality and hospital and intensive care unit lengths of stay decreased over time (P < 0.001), whereas the ARDS case-fatality did not change significantly.
Conclusions: despite an increase in patients' severity of illness, number of comorbidities, and prevalence of major ARDS risk factors, the incidence of ARDS in this suburban community decreased by more than half. Correlation of the observed findings with changes in health care delivery may have important implications for the planning of acute care services in other regions.
Figures



Comment in
-
Better supportive care, less ARDS: just do it?Am J Respir Crit Care Med. 2011 Jan 1;183(1):6-7. doi: 10.1164/rccm.201007-1139ED. Am J Respir Crit Care Med. 2011. PMID: 21193784 No abstract available.
References
-
- Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, Stern EJ, Hudson LD. Incidence and outcomes of acute lung injury. N Engl J Med 2005;353:1685–1693. - PubMed
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet 1967;2:319–323. - PubMed
-
- Luhr OR, Antonsen K, Karlsson M, Aardal S, Thorsteinsson A, Frostell CG, Bonde J. Incidence and mortality after acute respiratory failure and acute respiratory distress syndrome in Sweden, Denmark, and Iceland. Am J Respir Crit Care Med 1999;159:1849–1861. - PubMed
-
- Bersten AD, Edibam C, Hunt T, Moran J. Incidence and mortality of acute lung injury and the acute respiratory distress syndrome in three Australian states. Am J Respir Crit Care Med 2002;165:443–448. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
