

Targeted delivery of amikacin into granuloma
- PMID: 20693382
- PMCID: PMC3029940
- DOI: 10.1164/rccm.200912-1888OC
Targeted delivery of amikacin into granuloma
Abstract
Rationale: Nontuberculous mycobacterial (NTM) infection is a growing problem in the United States and remains underrecognized in the developing world. The management of NTM infections is further complicated by several factors, including the need to use high systemic doses of toxic agents, the length of therapy, and the development of drug resistance.
Objectives: We have evaluated the use of monocyte-derived dendritic cells (DCs) as a delivery vehicle for a luminescent derivative of amikacin prepared by conjugation to fluorescein isothiocyanate (FITC) (amikacin-FITC) into granulomas formed in the tissues of mice infected with Mycobacterium avium.
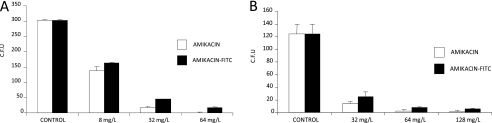
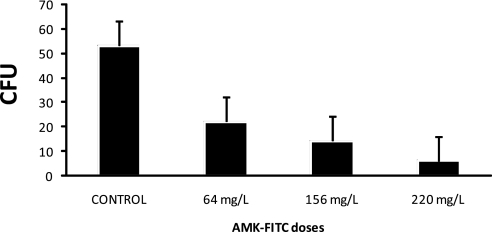
Methods: Amikacin-FITC was prepared and quantitative fluorescence was used to track the intracellular uptake of this modified antibiotic. The antibiotic activity of amikacin-FITC was also determined to be comparable to unmodified amikacin against M. avium. Amikacin-FITC-loaded DCs were first primed with M. avium, and then the cells were injected into the tail vein of infected mice. After 24 hours, the mice were sacrificed and the tissues were analyzed under fluorescence microscope.
Measurements and main results: We found that we were able to deliver amikacin into granulomas in a mouse model of disseminated mycobacterial infection. No increase in levels of monocyte chemoattractant protein-1 and its CCR2 as markers of inflammation were found when DCs were treated with amikacin-FITC.
Conclusions: DC-based drug delivery may be an adjunct and useful method of delivering high local concentrations of antibiotics into mycobacterial granulomas.
Figures









Comment in
-
A trojan horse strategy to deliver amikacin to mycobacterial granulomas.Am J Respir Crit Care Med. 2011 Oct 1;184(7):860; author reply 860-1. doi: 10.1164/ajrccm.184.7.860. Am J Respir Crit Care Med. 2011. PMID: 21965019 No abstract available.
References
-
- Steinman RM. The dendritic cell system and its role in immunogenicity. Annu Rev Immunol 1991;9:271–296. - PubMed
-
- Banchereau J, Steinman RM. Dendritic cells and the control of immunity. Nature 1998;392:245–252. - PubMed
-
- Mohagheghpour N, Gammon D, Kawamura LM, van Vollenhoven A, Benike CJ, Engleman EG. CTL response to Mycobacterium tuberculosis: identification of an immunogenic epitope in 19-kDa lipoprotein. J Immunol 1998;161:2400–2406. - PubMed
-
- Sprent J, Schaefer M. Antigen-presenting cells for unprimed T cells. Immunol Today 1989;10:17–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
