

Real-time hemodynamic assessment of downstream effects of intracranial stenoses in patients with orthostatic hypoperfusion syndrome
- PMID: 20693790
- PMCID: PMC3014861
- DOI: 10.1159/000319567
Real-time hemodynamic assessment of downstream effects of intracranial stenoses in patients with orthostatic hypoperfusion syndrome
Abstract
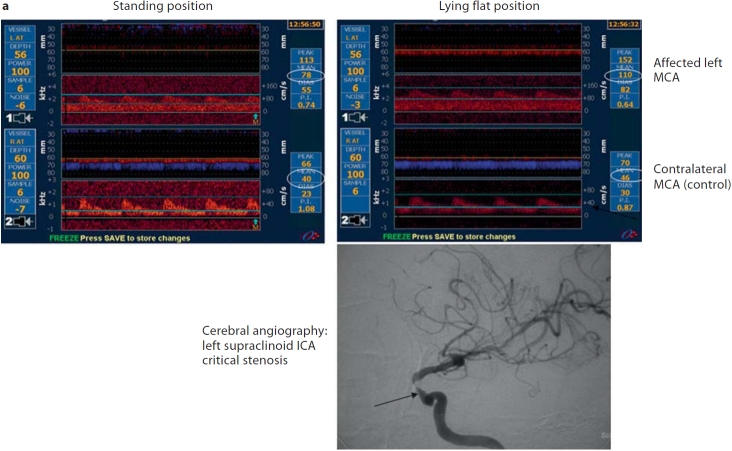
Background: Arterial flow velocity changes on transcranial Doppler can reflect changes in cerebral flow during position-induced ischemia if obtained during short-term monitoring of positional changes.
Subjects and methods: Our multicenter group monitored symptomatic and asymptomatic arteries in patients with recurrent neurological deficits during positional changes and documented intracranial arterial stenosis. Bilateral posterior cerebral and middle cerebral arteries were monitored dependent on clinical symptom localization. The symptomatic artery was monitored distal to the intracranial stenosis, and mean flow velocities (MFV) were recorded at different body positions. The symptomatic artery relative MFV ratio was defined as the ratio of symptomatic artery MFV in the asymptomatic position--MFV in the symptomatic position/MFV in the asymptomatic position.
Results: Sixteen patients underwent transcranial Doppler monitoring: mean age 62 +/- 19 years, 11 (69%) men, 6 (40%) with transient ischemic attacks. Ten patients (63%) had posterior and 6 anterior circulation symptoms. Patients developed neurological symptoms while standing up (63%) and/or sitting (44%), walking (13%) or during neck extension (6%). Symptomatic artery MFV dropped by > or =25% from the resting to the symptomatic position in all patients except for one. The mean symptomatic artery MFV relative ratio was higher compared with the mean asymptomatic artery MFV relative ratio: 0.5 +/- 0.28 versus -0.02 +/- 0.1 (p = 0.001, Wilcoxon test). The symptomatic artery relative ratio of >0.25 had a 94% sensitivity and 100% specificity for predicting neurological symptom development during testing (kappa = 0.9, p < 0.001).
Conclusions: A significant reduction in intracranial flow velocity distal to an intracranial stenosis can identify patients whose symptoms can worsen with positional changes. These patients may prove a target for interventional revascularization techniques.
Copyright (c) 2010 S. Karger AG, Basel.
Figures


References
-
- Warlow CP, Morris PJ. Transient Ischemic Attacks. New York: Marcel Dekker; 1982.
-
- Ruff RL, Talman WT, Petito F. Transient ischemic attacks associated with hypotension in hypertensive patients with carotid artery stenosis. Stroke. 1981;12:353–355. - PubMed
-
- Caplan LR, Wong KS, Gao S, Hennerici MG. Is hypoperfusion an important cause of strokes? If so, how? Cerebrovasc Dis. 2006;21:145–153. - PubMed
-
- Somerville ER. Orthostatic transient ischemic attacks: a symptom of large vessel occlusion. Stroke. 1984;15:1066–1067. - PubMed
-
- Pascual-Leone A, Anderson DC, Larson DA. Volume therapy in orthostatic transient ischemic attacks. Stroke. 1989;20:1267–1270. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
