

Antegrade balloon occlusion of inferior vena cava during thrombectomy for renal cell carcinoma
- PMID: 20694087
- PMCID: PMC2911982
- DOI: 10.5489/cuaj.892
Antegrade balloon occlusion of inferior vena cava during thrombectomy for renal cell carcinoma
Abstract
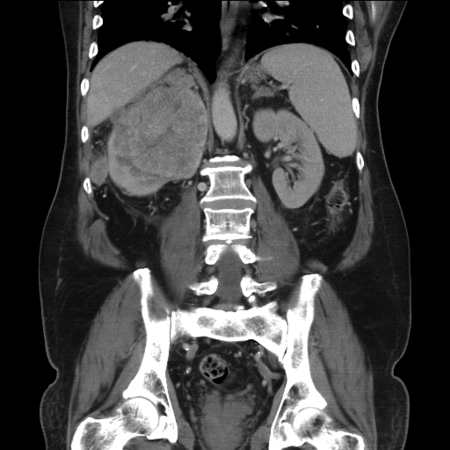
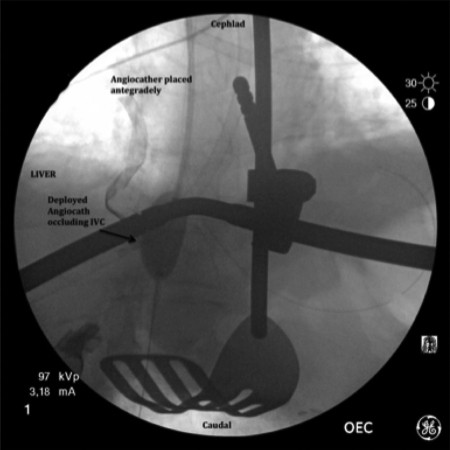
Nephrectomy with inferior vena cava (IVC) thrombectomy for advanced renal cell carcinoma (RCC) is a challenging and morbid surgical case. We describe the use of a simple endoluminal technique to occlude the suprahepatic IVC during thrombectomy. A 60-year-old male presented with a large right-sided RCC and IVC tumour thrombus. The tip of the thrombus, which was non-adherent to the caval wall, extended to the level of the hepatic veins. After complete dissection of the kidney, we obtained suprahepatic control of the IVC by a large compliant balloon, introduced through the right internal jugular vein and inflated just below the level of the diaphragm. The IVC thrombectomy was performed in a bloodless field. Mean blood pressure remained stable during IVC balloon inflation with a total occlusion time of 10 minutes. Intraprocedural completion cavogram and postoperative Doppler ultrasonography showed no residual IVC clot. Blood loss during the thrombectomy portion of the case was scant. The patient's postoperative course was uncomplicated and, at the last follow-up, he had stable metastatic disease on sunitinib therapy. For the surgical treatment of RCC with retrohepatic IVC tumour extension, transjugular balloon occlusion of the suprahepatic IVC offers an alternative to extensive hepatic mobilization to obtain suprahepatic thrombus control. Advantages over traditional surgical methods may include decreased surgical time, lower risk of liver injury and tumour embolism. We suggest this method for further evaluation.
Figures

Similar articles
-
Endoluminal occlusion of the inferior vena cava in renal cell carcinoma with retro- or suprahepatic caval thrombus.BJU Int. 2006 Jun;97(6):1216-20. doi: 10.1111/j.1464-410X.2006.06168.x. BJU Int. 2006. PMID: 16686714
-
Results of endoluminal occlusion of the inferior vena cava during radical nephrectomy and thrombectomy.Eur Urol. 2008 Oct;54(4):778-83. doi: 10.1016/j.eururo.2008.05.016. Epub 2008 May 27. Eur Urol. 2008. PMID: 18524467
-
Balloon control of the suprahepatic inferior vena cava: a novel technique for renal cell carcinoma tumor thrombus.Ann Vasc Surg. 2008 Mar;22(2):200-2. doi: 10.1016/j.avsg.2007.12.003. Ann Vasc Surg. 2008. PMID: 18346572
-
Robot-assisted hepatic mobilization and control of suprahepatic infradiaphragmatic inferior vena cava for level 3 vena caval thrombectomy: An IDEAL stage 0 study.J Surg Oncol. 2015 Dec;112(7):741-5. doi: 10.1002/jso.23980. Epub 2015 Aug 11. J Surg Oncol. 2015. PMID: 26265131 Review.
-
Important surgical considerations in the management of renal cell carcinoma (RCC) with inferior vena cava (IVC) tumour thrombus.BJU Int. 2012 Oct;110(7):926-39. doi: 10.1111/j.1464-410X.2012.11174.x. Epub 2012 Apr 30. BJU Int. 2012. PMID: 22540179 Review.
Cited by
-
Modified technique of cavoatrial tumor thrombectomy without cardiopulmonary by-pass and hypothermic circulatory arrest: a preliminary report.Cent European J Urol. 2015;68(3):311-7. doi: 10.5173/ceju.2015.588. Epub 2015 Aug 21. Cent European J Urol. 2015. PMID: 26568872 Free PMC article.
-
Surgical management of renal cell carcinoma: Canadian Kidney Cancer Forum Consensus.Can Urol Assoc J. 2014 May;8(5-6):E398-412. doi: 10.5489/cuaj.1894. Can Urol Assoc J. 2014. PMID: 25024794 Free PMC article. No abstract available.
-
Successful thrombectomy for inferior vena cava thrombosis associated with an ovarian tumor: a case report.J Surg Case Rep. 2025 Apr 5;2025(4):rjaf196. doi: 10.1093/jscr/rjaf196. eCollection 2025 Apr. J Surg Case Rep. 2025. PMID: 40191659 Free PMC article.
-
Vena cava balloon occlusion for pulmonary embolism prevention during resection of giant uterus fibroids.J Surg Case Rep. 2022 May 25;2022(5):rjac234. doi: 10.1093/jscr/rjac234. eCollection 2022 May. J Surg Case Rep. 2022. PMID: 35665394 Free PMC article.
-
Treatment of iatrogenic IVC occlusion with implantation of a stent of a new shape dedicated to aortic aneurysms.Pol J Radiol. 2013 Jan;78(1):75-7. doi: 10.12659/PJR.883772. Pol J Radiol. 2013. PMID: 23493805 Free PMC article.
References
-
- Pagano F, Dal Bianco M, Artibani W, et al. Renal cell carcinoma with extension into the inferior vena cava: Problems in diagnosis, staging and treatment. Eur Urol. 1992;22:200–3. - PubMed
-
- Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA.Campbell-Walsh Urology 9th editionPhiladelphia, PA: Saunders; 2007:table 47–15.
-
- Blute ML, Leibovich BC, Lohse CM, et al. The Mayo Clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. BJU Int. 2004;94:33–41. - PubMed
-
- Jibiki M, Iwai T, Inoue Y, et al. Surgical strategy for treating renal cell carcinoma with thrombus extending into the inferior vena cava. J Vasc Surg. 2004;39:829–35. - PubMed
-
- Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5:649–55. - PubMed
LinkOut - more resources
Full Text Sources
