

The effect of antipsychotic medication on neuromotor abnormalities in neuroleptic-naive nonaffective psychotic patients: a naturalistic study with haloperidol, risperidone, or olanzapine
- PMID: 20694120
- PMCID: PMC2911000
- DOI: 10.4088/PCC.09m00799gry
The effect of antipsychotic medication on neuromotor abnormalities in neuroleptic-naive nonaffective psychotic patients: a naturalistic study with haloperidol, risperidone, or olanzapine
Abstract
Objective: To examine the effect of antipsychotic medication on neuromotor abnormalities in a sample of psychotic patients never exposed to antipsychotic drugs.
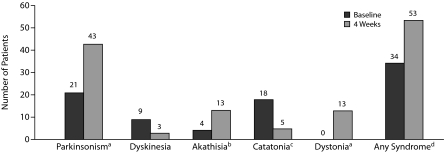
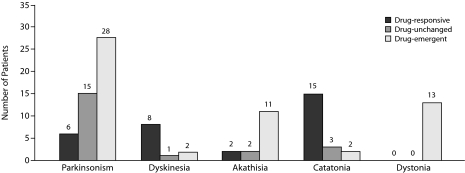
Method: One hundred psychotic patients were assessed (from January 1998 to December 2002) using DSM-IV criteria for parkinsonism, dyskinesia, akathisia, catatonia, and dystonia at baseline and after 4 weeks of treatment with haloperidol (n = 23), risperidone (n = 52), or olanzapine (n = 25). We examined change scores in neuromotor ratings over the treatment period across treatment groups and rates of drug-responsive and drug-emergent neuromotor syndromes in patients with and without preexisting neuromotor abnormalities.
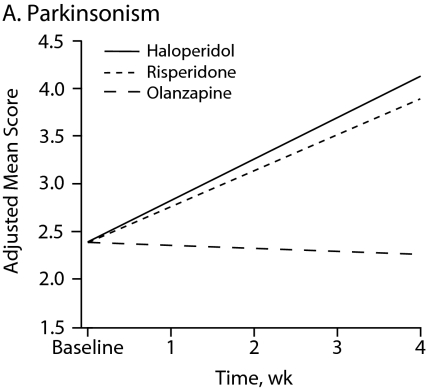
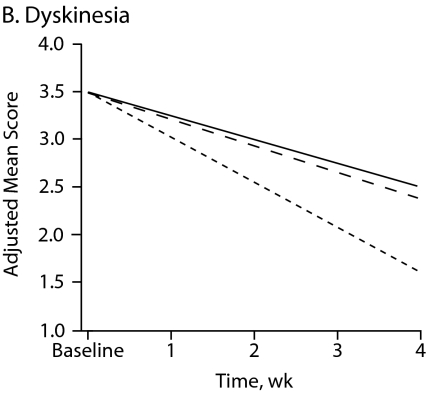
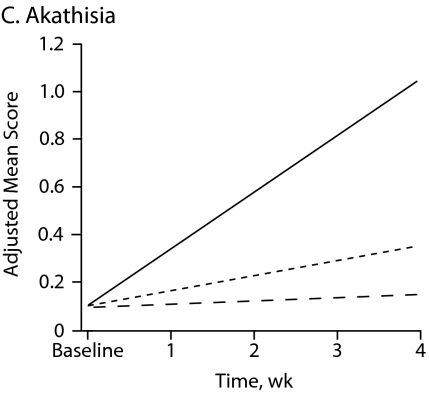
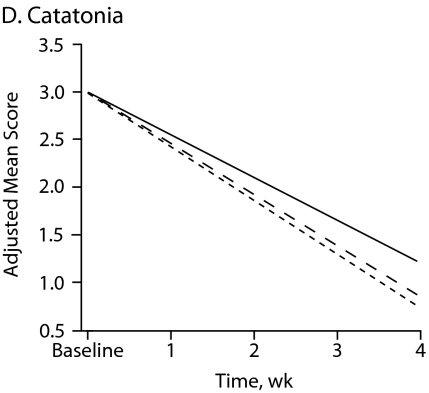
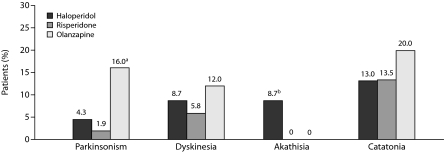
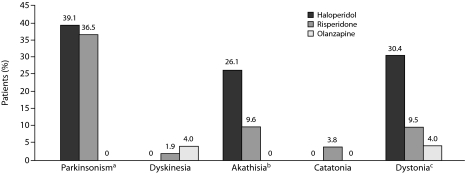
Results: Overall time effects revealed a worsening of parkinsonism (P = .002) and akathisia (P = .002) ratings and an improvement of dyskinesia (P = .001) and catatonia (P < .001) ratings. Main treatment effects revealed that patients taking haloperidol had a significant mean increase in akathisia scores compared with those of patients taking risperidone (P = .002) or olanzapine (P < .001). A significantly greater percentage of olanzapine-treated patients experienced remission of preexisting parkinsonism than did the other treatment groups (P = .047). Patients without preexisting motor abnormalities were more likely to experience drug-emergent parkinsonism if they were treated with haloperidol or risperidone than with olanzapine (P = .001) and were more likely to experience drug-emergent dystonia (P = .014) and akathisia (P = .013) if they were treated with haloperidol than with risperidone or olanzapine.
Conclusions: The relationship between antipsychotic medication and neurologic abnormalities is more complex than previously acknowledged since antipsychotic drugs may both improve preexisting abnormalities and cause "de novo" neurologic syndromes. Overall, olanzapine has a more favorable neuromotor profile than risperidone, which in turn has a more favorable profile than haloperidol.
Figures
Similar articles
-
An integrated analysis of acute treatment-emergent extrapyramidal syndrome in patients with schizophrenia during olanzapine clinical trials: comparisons with placebo, haloperidol, risperidone, or clozapine.J Clin Psychiatry. 2003 Aug;64(8):898-906. doi: 10.4088/jcp.v64n0807. J Clin Psychiatry. 2003. PMID: 12927004
-
A practical clinical trial comparing haloperidol, risperidone, and olanzapine for the acute treatment of first-episode nonaffective psychosis.J Clin Psychiatry. 2006 Oct;67(10):1511-21. doi: 10.4088/jcp.v67n1004. J Clin Psychiatry. 2006. PMID: 17107241 Clinical Trial.
-
Long-term antipsychotic monotherapy for schizophrenia: disease burden and comparative outcomes for patients treated with olanzapine, quetiapine, risperidone, or haloperidol monotherapy in a pan-continental observational study.J Clin Psychiatry. 2008 Dec;69(12):1901-15. Epub 2008 Sep 9. J Clin Psychiatry. 2008. PMID: 19012820
-
[Antipsychotics in bipolar disorders].Encephale. 2004 Sep-Oct;30(5):417-24. doi: 10.1016/s0013-7006(04)95456-5. Encephale. 2004. PMID: 15627046 Review. French.
-
[Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation].Encephale. 2005 Mar-Apr;31(2):235-46. doi: 10.1016/s0013-7006(05)82390-5. Encephale. 2005. PMID: 15959450 Review. French.
Cited by
-
Extrapyramidal symptoms predict cognitive performance after first-episode psychosis.Schizophrenia (Heidelb). 2022 Aug 4;8(1):64. doi: 10.1038/s41537-022-00270-8. Schizophrenia (Heidelb). 2022. PMID: 35927423 Free PMC article.
-
Aberrant Hyperconnectivity in the Motor System at Rest Is Linked to Motor Abnormalities in Schizophrenia Spectrum Disorders.Schizophr Bull. 2017 Sep 1;43(5):982-992. doi: 10.1093/schbul/sbx091. Schizophr Bull. 2017. PMID: 28911049 Free PMC article.
-
Motor Abnormalities: From Neurodevelopmental to Neurodegenerative Through "Functional" (Neuro)Psychiatric Disorders.Schizophr Bull. 2017 Sep 1;43(5):956-971. doi: 10.1093/schbul/sbx089. Schizophr Bull. 2017. PMID: 28911050 Free PMC article. Review.
-
Motor Behavior is Relevant for Understanding Mechanism, Bolstering Prediction, And Improving Treatment: A Transdiagnostic Perspective.Schizophr Bull. 2022 Jun 21;48(4):741-748. doi: 10.1093/schbul/sbac003. Schizophr Bull. 2022. PMID: 35137227 Free PMC article. No abstract available.
-
Characterization of spontaneous Parkinsonism in drug-naive patients with nonaffective psychotic disorders.Eur Arch Psychiatry Clin Neurosci. 2012 Mar;262(2):131-8. doi: 10.1007/s00406-011-0219-1. Epub 2011 May 28. Eur Arch Psychiatry Clin Neurosci. 2012. PMID: 21626260
References
-
- Kraepelin E. In: Dementia Praecox and Paraphrenia. Barclay RM, trans. Robertson GM, editor. NY: Huntington; Robert E. Krieger Publishing Co Inc; 1971.
-
- Bleuler E. In: Dementia Praecox or the Group of Schizophrenias. Zinkin J, editor. New York, NY: International University Press; 1950. trans.
-
- Leonhard K. Afteilung der endogen Psychosen. Berlin, Germany: Akademie Verlag; 1957. [The classification of endogenous psychoses]
-
- Friedman JH. Historical perspective on movement disorders. J Clin Psychiatry. 2004;65(suppl 9):3–8. - PubMed
-
- Ayd FJ. A survey of drug-induced extrapyramidal reactions. JAMA. 1961;175:1054–1060. - PubMed
LinkOut - more resources
Full Text Sources