

Hospital economics of primary total knee arthroplasty at a teaching hospital
- PMID: 20694537
- PMCID: PMC3008872
- DOI: 10.1007/s11999-010-1486-2
Hospital economics of primary total knee arthroplasty at a teaching hospital
Abstract
Background: The hospital cost of total knee arthroplasty (TKA) in the United States is a major growing expense for the Centers for Medicare & Medicaid Services (CMS). Many hospitals are unable to deliver TKA with profitable or breakeven economics under the current Diagnosis-Related Group (DRG) hospital reimbursement system.
Questions/purposes: The purposes of the current study were to (1) determine revenue, expenses, and profitability (loss) for TKA for all patients and for different payors; (2) define changes in utilization and unit costs associated with this operation; and (3) describe TKA cost control strategies to provide insight for hospitals to improve their economic results for TKA.
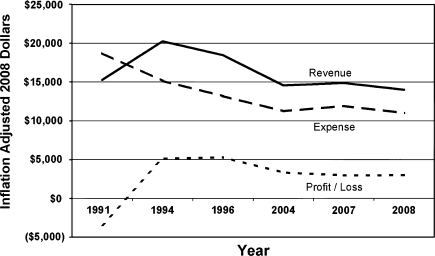
Results: From 1991 to 2009, Lahey Clinic converted a $2172 loss per case on primary TKA in 1991 to a $2986 profit per case in 2008. The improved economics was associated with decreasing revenue in inflation-adjusted dollars and implementation of hospital cost control programs that reduced hospital expenses for TKA. Reduction of hospital length of stay and reduction of knee implant costs were the major drivers of hospital expense reduction.
Conclusions: During the last 25 years, our economic experience with TKA is concerning. Hospital revenues have lagged behind inflation, hospital expenses have been reduced, and our institution is earning a profit. However, the margin for TKA is decreasing and Managed Medicare patients do not generate a profit. The erosion of hospital revenue for TKA will become a critical issue if it leads to economic losses for hospitals or reduced access to TKA.
Level of evidence: Level III, Economic and Decision Analyses. See Guidelines for Authors for a complete description of levels of evidence.
Figures
References
-
- Healy WL, Finn D. The hospital cost and the cost of the implant for total knee arthroplasty: a comparison between 1983 and 1991 for one hospital. J Bone Joint Surg Am. 1994;76:801–806. - PubMed
-
- Healy WL, Iorio R. Implant selection and cost for total joint arthroplasty: conflict between surgeons and hospitals. Clin Orthop Relat Res. 2007;457:57–63. - PubMed
-
- Healy WL, Iorio R, Ko J, Appleby D, Lemos DW. Impact of cost reduction programs on short-term patient outcome and hospital cost of total knee arthroplasty. J Bone Joint Surg Am. 2002;84:348–353. - PubMed
-
- Healy WL, Iorio R, Lemos MJ, Patch DA, Pfeifer BA, Smiley PM, Wilk RM. Single price/case price purchasing in orthopaedic surgery: experience at the Lahey Clinic. J Bone Joint Surg Am. 2000;82:607–612. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
