

Multicenter study of Clostridium difficile infection rates from 2000 to 2006
- PMID: 20695799
- PMCID: PMC3648217
- DOI: 10.1086/656245
Multicenter study of Clostridium difficile infection rates from 2000 to 2006
Abstract
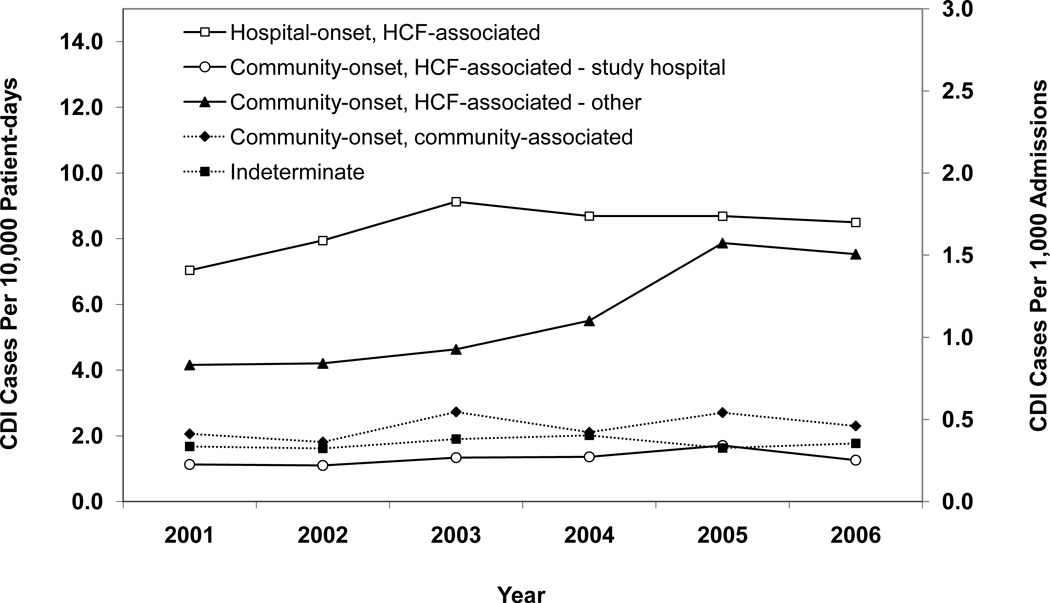
Objective: To compare incidence rates of Clostridium difficile infection (CDI) during a 6-year period among 5 geographically diverse academic medical centers across the United States by use of recommended standardized surveillance definitions of CDI that incorporate recent information on healthcare facility (HCF) exposure.
Methods: Data on C. difficile toxin assay results and dates of hospital admission and discharge were collected from electronic databases. Chart review was performed for patients with a positive C. difficile toxin assay result who were identified within 48 hours after hospital admission to determine whether they had any HCF exposure during the 90 days prior to their hospital admission. CDI cases, defined as any inpatient with a stool toxin assay positive for C. difficile, were categorized into 5 surveillance definitions based on recent HCF exposure. Annual CDI rates were calculated and evaluated by use of the chi(2) test for trend and the chi(2) summary test.
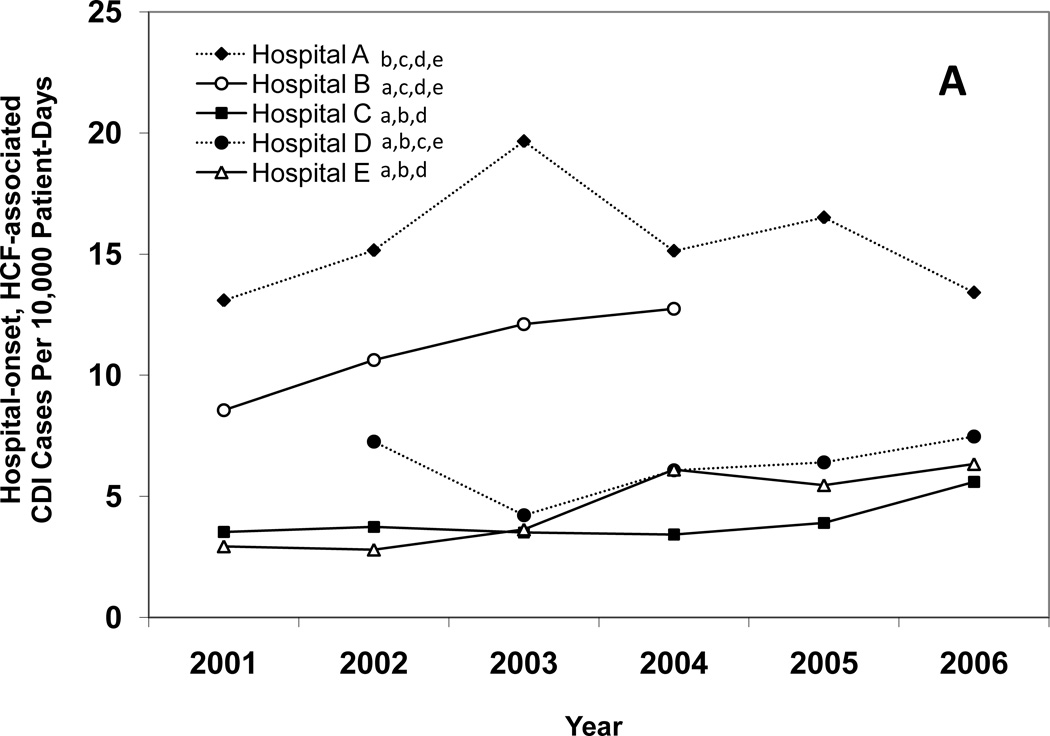
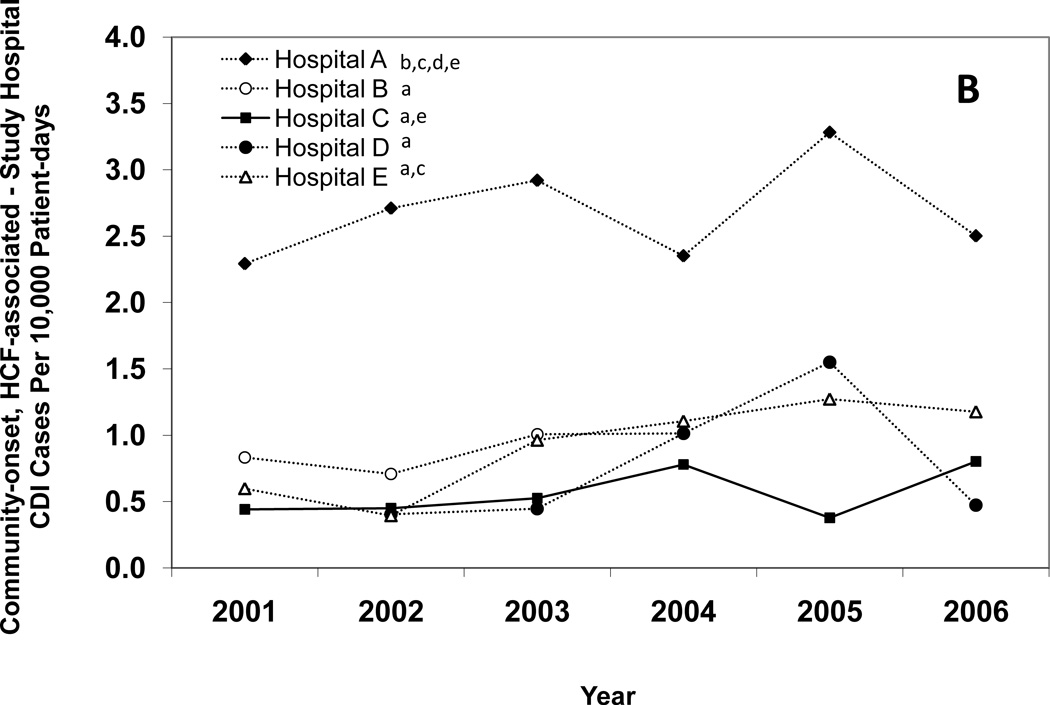
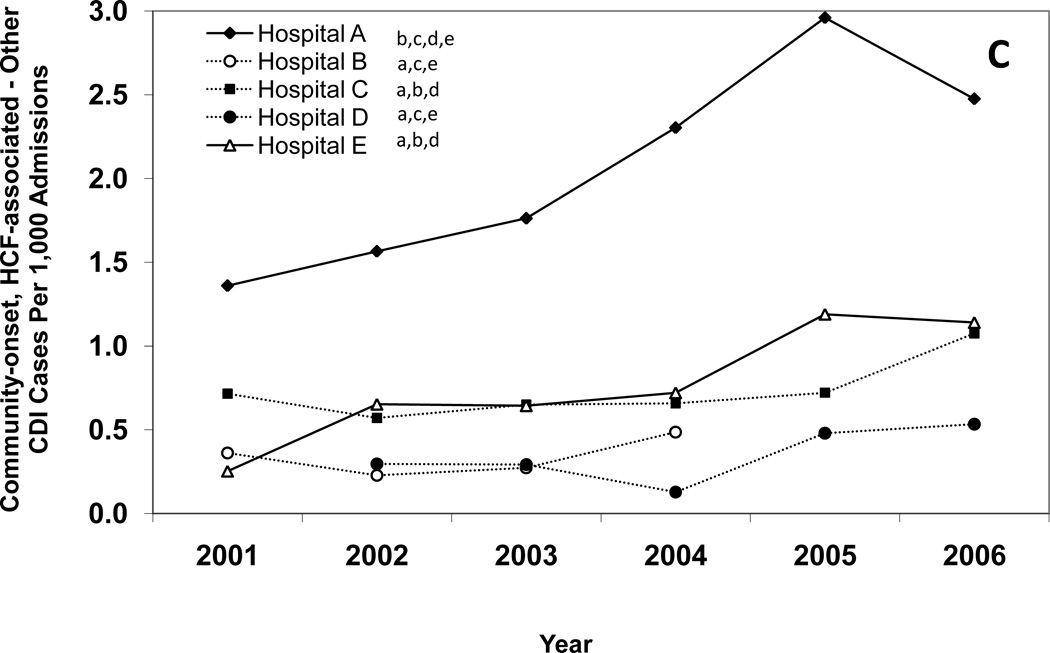
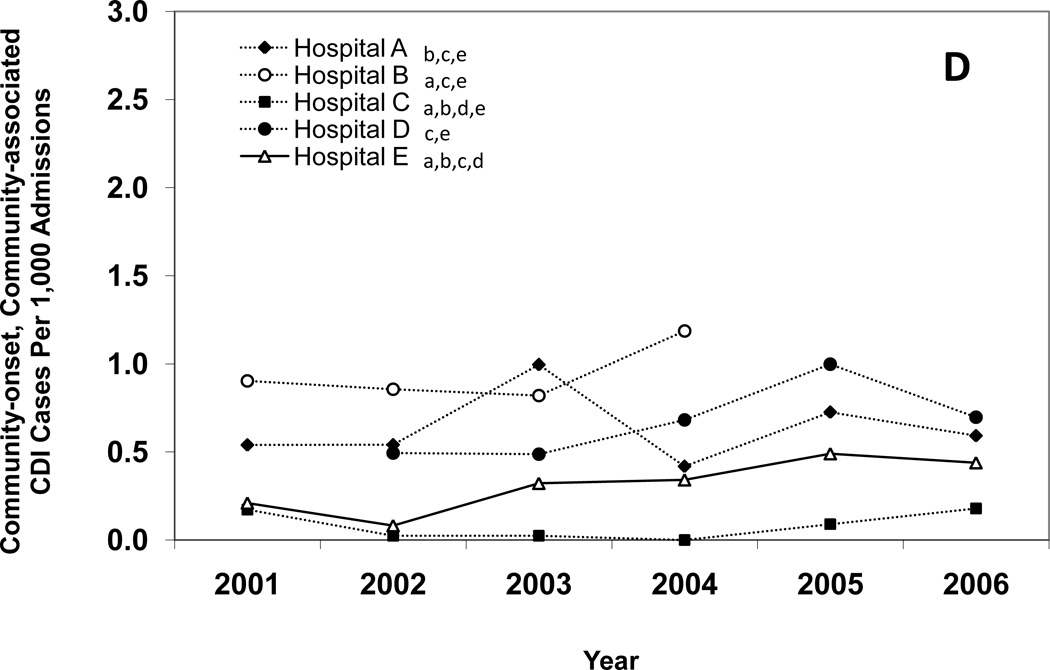
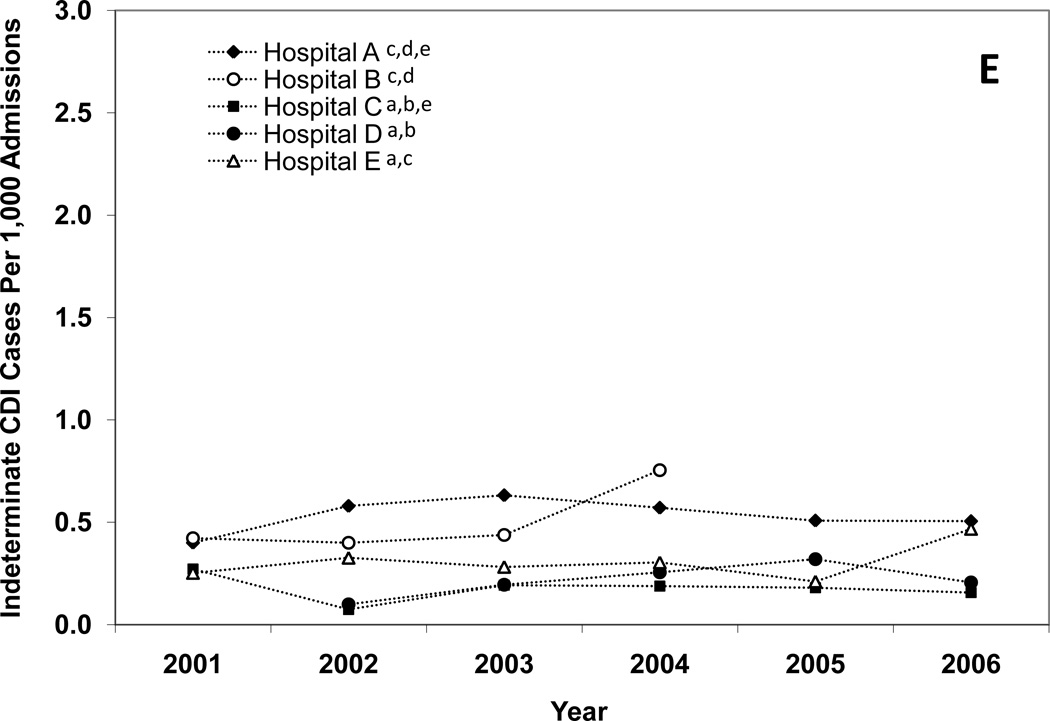
Results: During the study period, there were significant increases in the overall incidence rates of HCF-onset, HCF-associated CDI (from 7.0 to 8.5 cases per 10,000 patient-days; P < .001); community-onset, HCF-associated CDI attributed to a study hospital (from 1.1 to 1.3 cases per 10,000 patient-days; P = .003); and community-onset, HCF-associated CDI not attributed to a study hospital (from 0.8 to 1.5 cases per 1,000 admissions overall; P < .001). For each surveillance definition of CDI, there were significant differences in the total incidence rate between HCFs.
Conclusions: The increasing incidence rates of CDI over time and across healthcare institutions and the correlation of CDI incidence in different surveillance categories suggest that CDI may be a regional problem and not isolated to a single HCF within a community.
Figures
Similar articles
-
Multicenter study of the impact of community-onset Clostridium difficile infection on surveillance for C. difficile infection.Infect Control Hosp Epidemiol. 2009 Jun;30(6):518-25. doi: 10.1086/597380. Infect Control Hosp Epidemiol. 2009. PMID: 19419269 Free PMC article.
-
Population-based surveillance of Clostridium difficile infection in Manitoba, Canada, by using interim surveillance definitions.Infect Control Hosp Epidemiol. 2009 Oct;30(10):945-51. doi: 10.1086/605719. Infect Control Hosp Epidemiol. 2009. PMID: 19732008
-
Hospital-associated Clostridium difficile infection: is it necessary to track community-onset disease?Infect Control Hosp Epidemiol. 2009 Apr;30(4):332-7. doi: 10.1086/596604. Infect Control Hosp Epidemiol. 2009. PMID: 19239377 Free PMC article.
-
The growing incidence and severity of Clostridium difficile infection in inpatient and outpatient settings.Expert Rev Gastroenterol Hepatol. 2010 Aug;4(4):409-16. doi: 10.1586/egh.10.48. Expert Rev Gastroenterol Hepatol. 2010. PMID: 20678014 Review.
-
Burden of Clostridioides difficile infection (CDI) - a systematic review of the epidemiology of primary and recurrent CDI.BMC Infect Dis. 2021 May 19;21(1):456. doi: 10.1186/s12879-021-06147-y. BMC Infect Dis. 2021. PMID: 34016040 Free PMC article.
Cited by
-
Fecal microbiota transplantation for the treatment of recurrent and severe Clostridium difficile infection in solid organ transplant recipients: A multicenter experience.Am J Transplant. 2019 Feb;19(2):501-511. doi: 10.1111/ajt.15058. Epub 2018 Aug 31. Am J Transplant. 2019. PMID: 30085388 Free PMC article.
-
Clostridium difficile ribotype does not predict severe infection.Clin Infect Dis. 2012 Dec;55(12):1661-8. doi: 10.1093/cid/cis786. Epub 2012 Sep 12. Clin Infect Dis. 2012. PMID: 22972866 Free PMC article.
-
Epidemiology of Clostridium difficile infection: results of a hospital-based study in Krakow, Poland.Epidemiol Infect. 2015 Nov;143(15):3235-43. doi: 10.1017/S0950268815000552. Epub 2015 Apr 10. Epidemiol Infect. 2015. PMID: 25858553 Free PMC article.
-
The dlt operon confers resistance to cationic antimicrobial peptides in Clostridium difficile.Microbiology (Reading). 2011 May;157(Pt 5):1457-1465. doi: 10.1099/mic.0.045997-0. Epub 2011 Feb 17. Microbiology (Reading). 2011. PMID: 21330441 Free PMC article.
-
Strategies to prevent Clostridioides difficile infections in acute-care hospitals: 2022 Update.Infect Control Hosp Epidemiol. 2023 Apr;44(4):527-549. doi: 10.1017/ice.2023.18. Infect Control Hosp Epidemiol. 2023. PMID: 37042243 Free PMC article. No abstract available.
References
-
- Gravel D, Miller M, Simor A, Taylor G, Gardam M, McGeer A, et al. Health care-associated Clostridium difficile infection in adults admitted to acute care hospitals in Canada: a Canadian Nosocomial Infection Surveillance Program Study. Clin Infect Dis. 2009;48(5):568–576. - PubMed
-
- Loo VG, Poirier L, Miller MA, Oughton M, Libman MD, Michaud S, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005;353(23):2442–2449. - PubMed
-
- McDonald LC, Killgore GE, Thompson A, Owens RC, Jr, Kazakova SV, Sambol SP, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med. 2005;353(23):2433–2441. - PubMed
Publication types
MeSH terms
Grants and funding
- UR8/CCU715087-06/1/PHS HHS/United States
- K01 AI065808/AI/NIAID NIH HHS/United States
- K23 AI065806/AI/NIAID NIH HHS/United States
- U01 CI000344/CI/NCPDCID CDC HHS/United States
- K01AI065808/AI/NIAID NIH HHS/United States
- K12RR02324901/RR/NCRR NIH HHS/United States
- 5U01CI000327/CI/NCPDCID CDC HHS/United States
- L30 AI062141/AI/NIAID NIH HHS/United States
- K24AI06779401/AI/NIAID NIH HHS/United States
- U01 CI000328/CI/NCPDCID CDC HHS/United States
- U01 CI000327/CI/NCPDCID CDC HHS/United States
- 5U01CI000328/CI/NCPDCID CDC HHS/United States
- 5U01CI000344/CI/NCPDCID CDC HHS/United States
- 5U01C1000333/PHS HHS/United States
- U01 CI000334/CI/NCPDCID CDC HHS/United States
LinkOut - more resources
Full Text Sources
Medical
