

Masked hypertension defined by ambulatory blood pressure monitoring is associated with an increased serum glucose level and urinary albumin-creatinine ratio
- PMID: 20695934
- PMCID: PMC5559301
- DOI: 10.1111/j.1751-7176.2010.00286.x
Masked hypertension defined by ambulatory blood pressure monitoring is associated with an increased serum glucose level and urinary albumin-creatinine ratio
Abstract
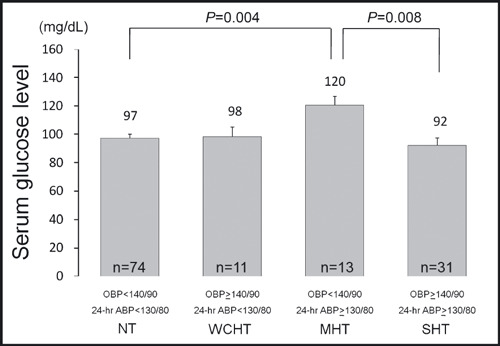
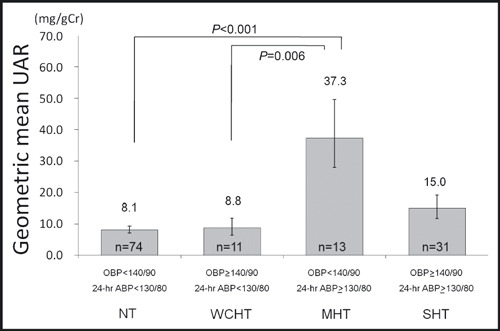
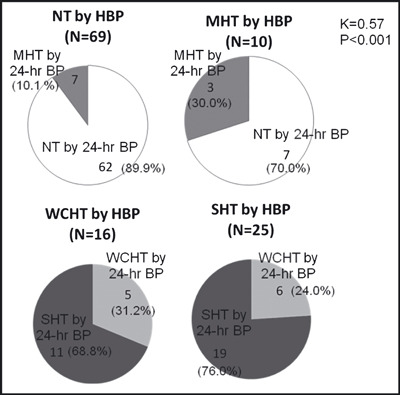
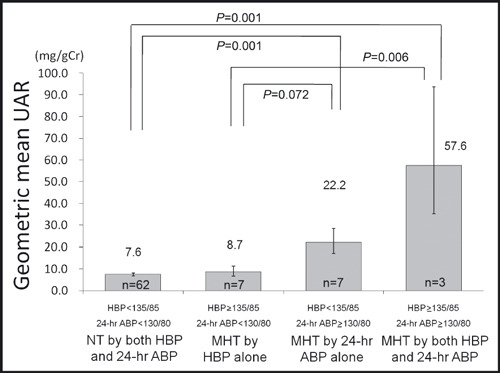
The authors evaluated the relationship of hypertensive target organ damage to masked hypertension assessed by ambulatory blood pressure (BP) and home blood pressure (HBP) monitoring in 129 participants without taking antihypertensive medication. Masked hypertension was defined as office BP < or =140/90 mm Hg and 24-hour ambulatory BP > or =130/80 mm Hg. The masked hypertensive participants defined by 24-hour ambulatory BP (n=13) had a higher serum glucose level (126 vs 96 mg/dL, P=.001) and urinary albumin-creatinine ratio (38.0 vs 7.5 mg/gCr, P<.001) than the normotensive participants (n=74); however, these relationships were not observed when the authors defined groups using HBP (> or =135/85 mm Hg). Masked hypertension by both 24-hour ambulatory BP and HBP had a higher urinary albumin-creatinine ratio than normotension by both 24-hour ambulatory BP and HBP (62.1 vs 7.4 mg/gCr, P=.001), and than masked hypertension by HBP alone (9.3 mg/gCr, P=.009). Masked hypertension defined by 24-hour ambulatory BP is associated with an increased serum glucose level and urinary albumin-creatinine ratio, but these relationships are not observed in masked hypertension defined by HBP.
Figures
Similar articles
-
Seasonal Variation of Home Blood Pressure and Its Association With Target Organ Damage: The J-HOP Study (Japan Morning Surge-Home Blood Pressure).Am J Hypertens. 2020 Jul 18;33(7):620-628. doi: 10.1093/ajh/hpaa027. Am J Hypertens. 2020. PMID: 32202625 Free PMC article.
-
Cardiovascular Event Risks Associated With Masked Nocturnal Hypertension Defined by Home Blood Pressure Monitoring in the J-HOP Nocturnal Blood Pressure Study.Hypertension. 2020 Jul;76(1):259-266. doi: 10.1161/HYPERTENSIONAHA.120.14790. Epub 2020 Jun 10. Hypertension. 2020. PMID: 32520613
-
Masked hypertension and target organ damage in treated hypertensive patients.Am J Hypertens. 2006 Sep;19(9):880-6. doi: 10.1016/j.amjhyper.2006.03.006. Am J Hypertens. 2006. PMID: 16942927
-
Clinical value of ambulatory blood pressure: evidence and limits.Circ Res. 2015 Mar 13;116(6):1034-45. doi: 10.1161/CIRCRESAHA.116.303755. Circ Res. 2015. PMID: 25767288 Review.
-
Changes in home versus clinic blood pressure with antihypertensive treatments: a meta-analysis.Hypertension. 2008 Nov;52(5):856-64. doi: 10.1161/HYPERTENSIONAHA.108.115600. Epub 2008 Sep 22. Hypertension. 2008. PMID: 18809791 Free PMC article.
Cited by
-
Blood pressure measurement: clinic, home, ambulatory, and beyond.Am J Kidney Dis. 2012 Sep;60(3):449-62. doi: 10.1053/j.ajkd.2012.01.026. Epub 2012 Apr 21. Am J Kidney Dis. 2012. PMID: 22521624 Free PMC article. Review.
-
Masked hypertension as an unrecognized destructive condition.J Clin Hypertens (Greenwich). 2014 Feb;16(2):155. doi: 10.1111/jch.12240. Epub 2013 Dec 12. J Clin Hypertens (Greenwich). 2014. PMID: 24330197 Free PMC article. No abstract available.
-
Inflammatory markers should be assessed together with cardiovascular risk factors by clinicians in masked hypertension.J Clin Hypertens (Greenwich). 2013 Jun;15(6):443-4. doi: 10.1111/jch.12120. Epub 2013 Apr 29. J Clin Hypertens (Greenwich). 2013. PMID: 23730994 Free PMC article. No abstract available.
-
Relationship between endothelial dysfunction and kidney disease.J Clin Hypertens (Greenwich). 2014 Feb;16(2):156. doi: 10.1111/jch.12236. Epub 2013 Dec 12. J Clin Hypertens (Greenwich). 2014. PMID: 24330143 Free PMC article. No abstract available.
-
Diagnostic performance of clinic and home blood pressure measurements compared with ambulatory blood pressure: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2020 Nov 23;20(1):491. doi: 10.1186/s12872-020-01736-2. BMC Cardiovasc Disord. 2020. PMID: 33225900 Free PMC article.
References
-
- Pickering TG, Davidson K, Gerin W, et al. Masked hypertension. Hypertension. 2002;40:795–796. - PubMed
-
- Pickering TG, Eguchi K, Kario K. Masked hypertension: a review. Hypertens Res. 2007;30:479–488. - PubMed
-
- Liu JE, Roman MJ, Pini R, et al. Cardiac and arterial target organ damage in adults with elevated ambulatory and normal office blood pressure. Ann Intern Med. 1999;131:564–572. - PubMed
-
- Sega R, Trocino G, Lanzarotti A, et al. Alterations of cardiac structure in patients with isolated office, ambulatory, or home hypertension: data from the general population (Pressione Arteriose Monitorate E Loro Associazioni [PAMELA] study). Circulation. 2001;104:1385–1392. - PubMed
-
- Ohkubo T, Kikuya M, Metoki H, et al. Prognosis of “masked” hypertension and “white‐coat” hypertension detected by 24‐h ambulatory blood pressure monitoring: 10‐year follow‐up from the Ohasama study. J Am Coll Cardiol. 2005;46:508–515. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
