

The cluster-randomized Quality Initiative in Rectal Cancer trial: evaluating a quality-improvement strategy in surgery
- PMID: 20696797
- PMCID: PMC2934795
- DOI: 10.1503/cmaj.091883
The cluster-randomized Quality Initiative in Rectal Cancer trial: evaluating a quality-improvement strategy in surgery
Abstract
Background: Following surgery for rectal cancer, two unfortunate outcomes for patients are permanent colostomy and local recurrence of cancer. We tested whether a quality-improvement strategy to change surgical practice would improve these outcomes.
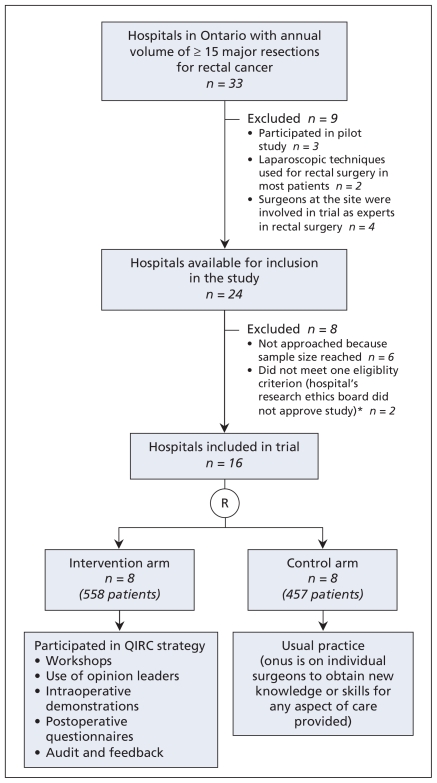
Methods: Sixteen hospitals were cluster-randomized to the intervention (Quality Initiative in Rectal Cancer strategy) or control (normal practice) arm. Consecutive patients with primary rectal cancer were accrued from May 2002 to December 2004. Surgeons at hospitals in the intervention arm could voluntarily participate by attending workshops, using opinion leaders, inviting a study team surgeon to demonstrate optimal techniques of total mesorectal excision, completing postoperative questionnaires, and receiving audits and feedback. Main outcome measures were hospital rates of permanent colostomy and local recurrence of cancer.
Results: A total of 56 surgeons (n = 558 patients) participated in the intervention arm and 49 surgeons (n = 457 patients) in the control arm. The median follow-up of patients was 3.6 years. In the intervention arm, 70% of surgeons participated in workshops, 70% in intraoperative demonstrations and 71% in postoperative questionnaires. Surgeons who had an intraoperative demonstration provided care to 86% of the patients in the intervention arm. The rates of permanent colostomy were 39% in the intervention arm and 41% in the control arm (odds ratio [OR] 0.97, 95% confidence interval [CI] 0.63-1.48). The rates of local recurrence were 7% in the intervention arm and 6% in the control arm (OR 1.06, 95% CI 0.68-1.64).
Interpretation: Despite good participation by surgeons, the resource-intense quality-improvement strategy did not reduce hospital rates of permanent colostomy or local recurrence compared with usual practice.
Trial registration: ClinicalTrials.gov NCT00182130.
Figures
Comment in
-
Mathematical models and cost-effective screening strategies for colorectal cancer.CMAJ. 2010 Sep 7;182(12):1283-4. doi: 10.1503/cmaj.100986. Epub 2010 Aug 16. CMAJ. 2010. PMID: 20713572 Free PMC article. No abstract available.
References
-
- Soreide O, Norstein J. Local recurrence after operative treatment of rectal carcinoma: a strategy for change. J Am Coll Surg. 1997;184:84–92. - PubMed
-
- Havenga K, Enker WE, DeRuiter MC, et al. Anatomical basis of total mesorectal excision and preservation of the pelvic autonomic nerves. In: Soreide O, Norstein J, editors. Rectal Cancer Surgery Optimisation, standardisation, documentation. New York (NY): Springer-Verlag; 1997. pp. 134–42.
-
- Bernstein MA, Amarnath B, Weiss EG, et al. Total mesorectal excision without adjuvant therapy for local control of rectal cancer: a North American experience. Tech Coloproctol. 1998;2:11–5.
-
- Arenas RB, Fichera A, Mhoon D, et al. Total mesenteric excision in the surgical treatment of rectal cancer: a prospective study. Arch Surg. 1998;133:608–12. - PubMed
-
- Heald RJ, Moran BJ, Ryall RDH, et al. The Basingstoke experience of total mesorectal excision. Arch Surg. 1998;133:894–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical