

Ambulatory antibiotic use and prescription drug coverage in older adults
- PMID: 20696953
- PMCID: PMC3784024
- DOI: 10.1001/archinternmed.2010.235
Ambulatory antibiotic use and prescription drug coverage in older adults
Abstract
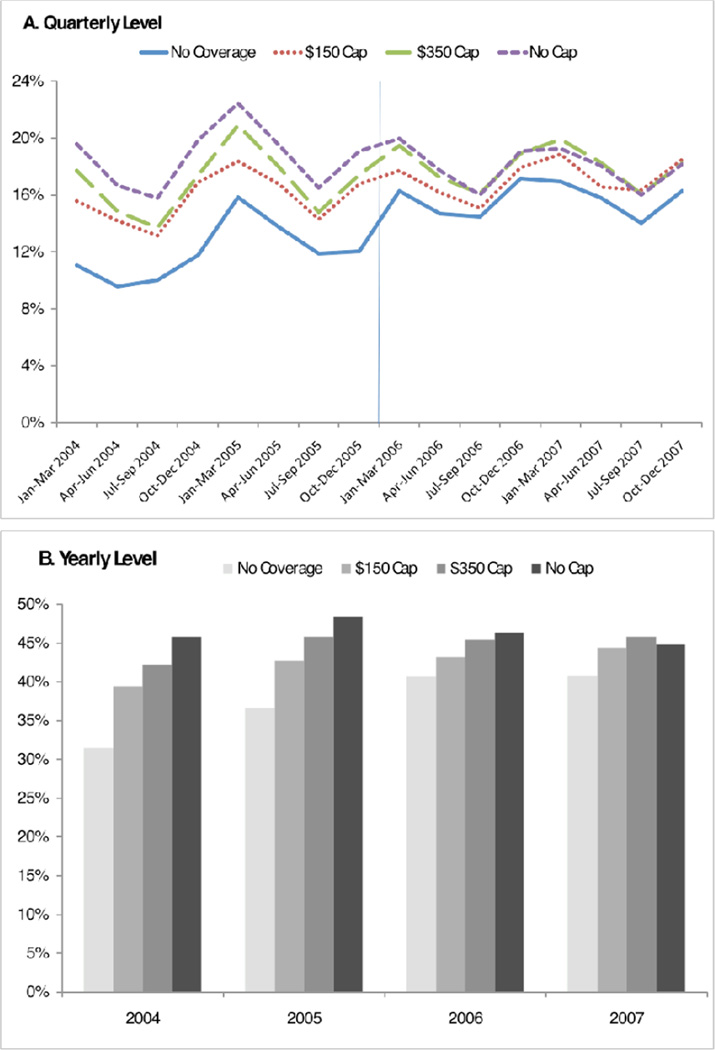
Background: Several studies have shown that use of medications to treat chronic conditions is highly sensitive to out-of-pocket price and influenced by changes in insurance coverage. Because antibiotics target infections and are used for a short period, one may expect antibiotic use to be less responsive to price. However, no studies have evaluated how antibiotic use changes with drug coverage. We evaluate changes in ambulatory oral antibiotic use after implementation of the Medicare drug benefit (Part D).
Methods: We conducted a comparison group analysis 2 years before and after implementation of Part D using insurance claims data from a large Medicare Advantage plan (January 1, 2004, through December 31, 2007). Outcomes included the likelihood of using any oral antibiotics and major antibiotic subclasses among 35 102 older adults and rates of antibiotic use among those with pneumonia and other acute respiratory tract infections.
Results: Overall antibiotic use increased most among those who did not previously have drug coverage (relative odds ratio [OR], 1.58; 95% confidence interval [CI], 1.36-1.85). Use of the broad spectrum antibiotic subclasses of quinolones (OR, 1.70; 95% CI, 1.35-2.15) and macrolides (1.59; 1.26-2.01) increased more than the use of other subclasses, especially for those with prior drug coverage. Rates of ambulatory antibiotic use associated with pneumonia increased (OR, 3.60; 95% CI, 2.35-5.53) more than those associated with other acute respiratory tract infections (2.29; 1.85-2.83).
Conclusions: Antibiotic use increased among older adults whose drug coverage improved after Part D implementation, with the largest increases for broad spectrum, newer, and more expensive antibiotics. Our study suggests reimbursement may play a role in addressing inappropriate antibiotic use.
Figures
Comment in
-
Decreasing out-of-pocket costs of antibiotics: the good, the bad, and the unknown.Arch Intern Med. 2010 Aug 9;170(15):1314-6. doi: 10.1001/archinternmed.2010.225. Arch Intern Med. 2010. PMID: 20696954 No abstract available.
References
-
- Arason VA, Sigurdsson JA, Erlendsdottir H, Gudmundsson S, Kristinsson KG. The role of antimicrobial use in the epidemiology of resistant pneumococci: A 10-year follow up. Microb Drug Resist. 2006;12(3):169–176. - PubMed
-
- Ranji SR, Steinman MA, Shojania KG, Gonzales R. Interventions to reduce unnecessary antibiotic prescribing: a systematic review and quantitative analysis. Med Care. 2008;46(8):847–862. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
