

Preventing potentially inappropriate medication use in hospitalized older patients with a computerized provider order entry warning system
- PMID: 20696957
- PMCID: PMC3638236
- DOI: 10.1001/archinternmed.2010.244
Preventing potentially inappropriate medication use in hospitalized older patients with a computerized provider order entry warning system
Abstract
Background: Potentially inappropriate medication (PIM) use in hospitalized older patients is common. Our objective was to determine whether a computerized provider order entry (CPOE) drug warning system can decrease orders for PIMs in hospitalized older patients.
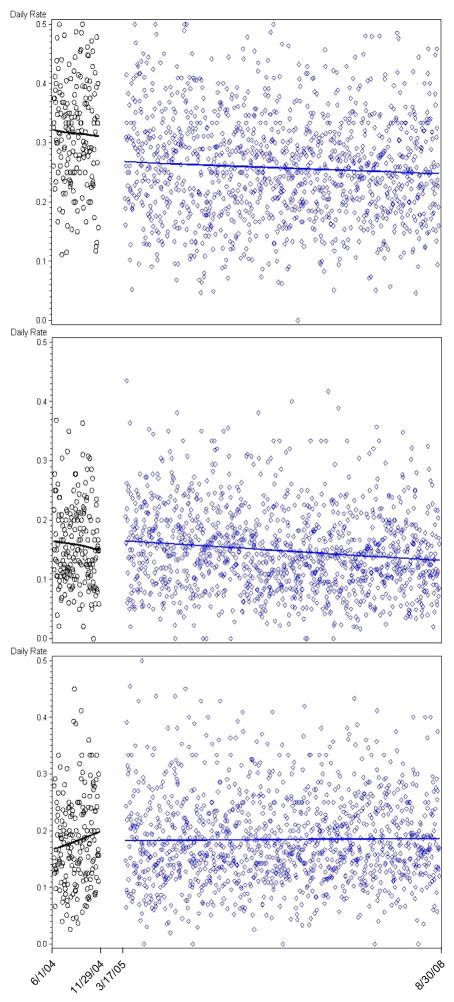
Methods: We used a prospective before-and-after design among patients 65 years or older admitted to a large, urban academic medical center in Boston, Massachusetts, from June 1, 2004, through November 29, 2004 (for patients admitted before the warning system was added), and from March 17, 2005, through August 30, 2008 (patients admitted after the warning system was added). We instituted a medication-specific warning system within CPOE that alerted ordering providers at the point of care when ordering a PIM and that advised alternative medication or dose reduction. The main outcome measure was the rate of orders for PIMs before and after the warning system was deployed.
Results: The mean (SE) rate of ordering medications that were not recommended dropped from 11.56 (0.36) to 9.94 (0.12) orders per day after the implementation of a CPOE warning system (difference, 1.62 [0.33]; P<.001), with no evidence that the effect waned over time. There were no appreciable changes in the rate of ordering medications for which only dose reduction was recommended or that were not targeted after CPOE implementation. These effects persisted in autoregressive models that accounted for secular trends and season (P<.001).
Conclusion: Specific alerts embedded into a CPOE system, used in patients 65 years or older, can decrease the number of orders of PIMs quickly and specifically.
Figures
Comment in
-
Time to change the paradigm--from "potentially inappropriate" to real patient harms.Arch Intern Med. 2011 Mar 14;171(5):473-4; author reply 474. doi: 10.1001/archinternmed.2011.48. Arch Intern Med. 2011. PMID: 21403049 No abstract available.
References
-
- Passarelli MC, Jacob-Filho W, Figueras A. Adverse drug reactions in an elderly hospitalised population: inappropriate prescription is a leading cause. Drugs Aging. 2005;22(9):767–777. - PubMed
-
- Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. Adverse Drug Events Prevention Study Group. JAMA. 1997 Jan 22–29;277(4):307–311. - PubMed
-
- Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 2003 Dec 8–22;163(22):2716–2724. - PubMed
-
- Onder G, Landi F, Cesari M, Gambassi G, Carbonin P, Bernabei R. Inappropriate medication use among hospitalized older adults in Italy: results from the Italian Group of Pharmacoepidemiology in the Elderly. Eur J Clin Pharmacol. 2003 Jun;59(2):157–162. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
