

Persistence with stroke prevention medications 3 months after hospitalization
- PMID: 20697032
- PMCID: PMC10197116
- DOI: 10.1001/archneurol.2010.190
Persistence with stroke prevention medications 3 months after hospitalization
Abstract
Objective: To measure longitudinal use of stroke prevention medications following stroke hospital discharge. We hypothesized that a combination of patient-, provider-, and system-level factors influence medication-taking behavior.
Design: Observational cohort design.
Setting: One hundred six US hospitals participating in the American Heart Association Get With The Guidelines-Stroke program.
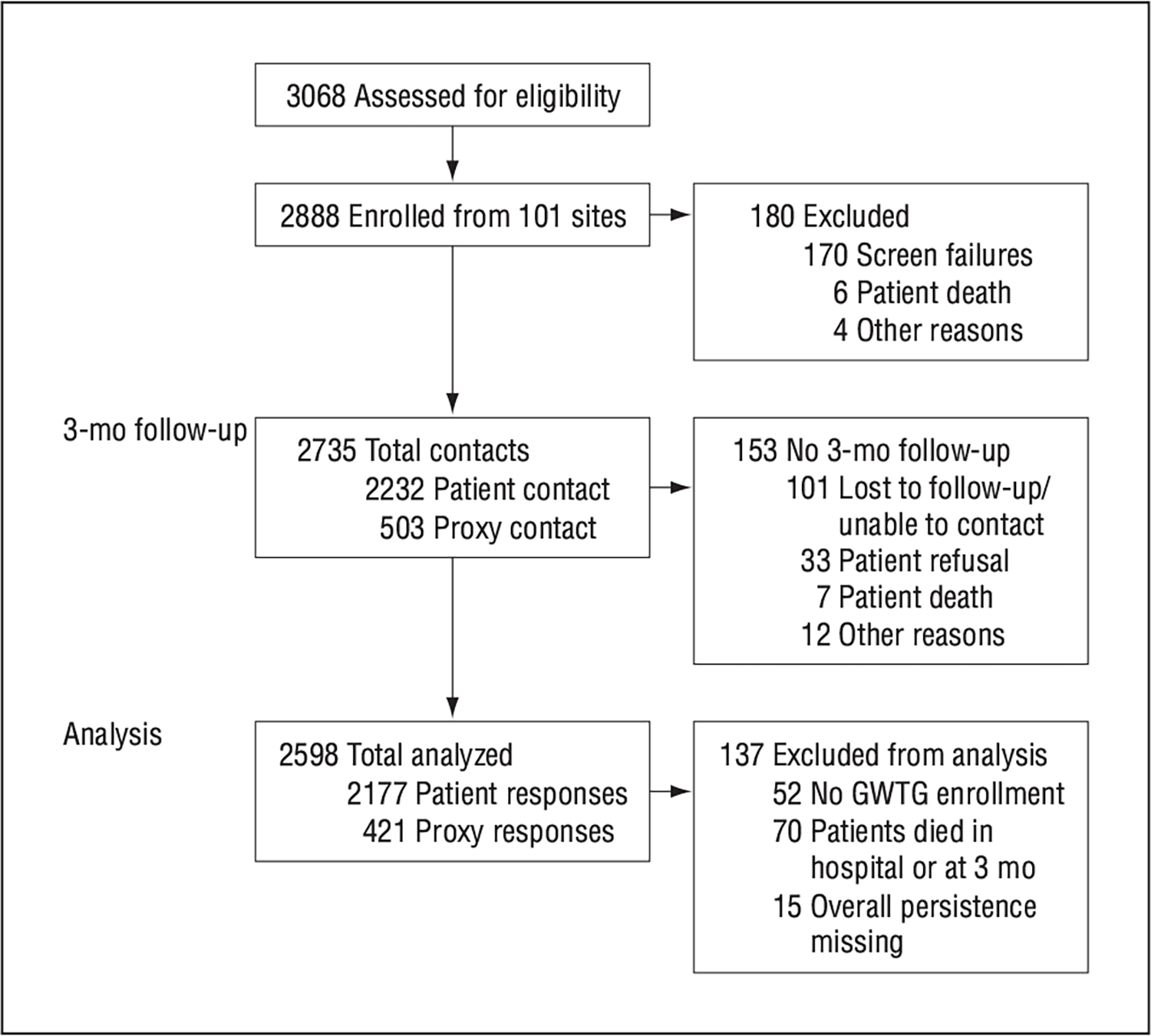
Patients: Two thousand eight hundred eighty-eight patients 18 years or older admitted with ischemic stroke or transient ischemic attack.
Main outcome measure: Regimen persistence, including use of antiplatelet therapies, warfarin, antihypertensive therapies, lipid-lowering therapies, or diabetes medications, from discharge to 3 months. Reasons for nonpersistence were also ascertained.
Results: Two thousand five hundred ninety-eight patients (90.0%) were eligible for analysis. At 3 months, 75.5% of subjects continued taking all secondary prevention medications prescribed at discharge. Persistence at 3 months was associated with decreasing number of medication classes prescribed, increasing age, medical history, less severe stroke disability, having insurance, working status, understanding why medications are prescribed and how to refill them, increased quality of life, financial hardship, geographic region, and hospital size.
Conclusions: One-quarter of stroke patients reported discontinuing 1 or more of their prescribed regimen of secondary prevention medications within 3 months of hospitalization for an acute stroke. Several modifiable factors associated with regimen persistence were identified and could be targets for improving long-term secondary stroke prevention.
Figures
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. ; Writing Group Members; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2010 update: a report from the American Heart Association [published correction appears in Circulation. 2010;121 (12):e260]. Circulation. 2010;121(7):e46–e215. doi: 36910.1161/CIRCULATI0NAHA.1109.192667. - PubMed
-
- Ovbiagele B, Saver JL, Fredieu A, et al. In-hospital initiation of secondary stroke prevention therapies yields high rates of adherence at follow-up. Stroke. 2004; 35(12):2879–2883. - PubMed
-
- Rahiman A, Saver JL, Porter V, et al. In-hospital initiation of secondary prevention is associated with improved vascular outcomes at 3 months. J Stroke Cerebrovasc Dis. 2008;17(1):5–8. - PubMed
-
- Ho PM, Spertus JA, Masoudi FA, et al. Impact of medication therapy discontinuation on mortality after myocardial infarction. Arch Intern Med. 2006;166(17):1842–1847. - PubMed
-
- De Schryver EL, van Gijn J, Kappelle LJ, Koudstaal PJ, Algra A; Dutch TIA trial and SPIRIT study groups. Non-adherence to aspirin or oral anticoagulants in secondary prevention after ischaemic stroke. J Neurol. 2005;252(11):1316–1321. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
