

Diagnosis-independent Alzheimer disease biomarker signature in cognitively normal elderly people
- PMID: 20697045
- PMCID: PMC2963067
- DOI: 10.1001/archneurol.2010.179
Diagnosis-independent Alzheimer disease biomarker signature in cognitively normal elderly people
Abstract
Objective: To identify biomarker patterns typical for Alzheimer disease (AD) in an independent, unsupervised way, without using information on the clinical diagnosis.
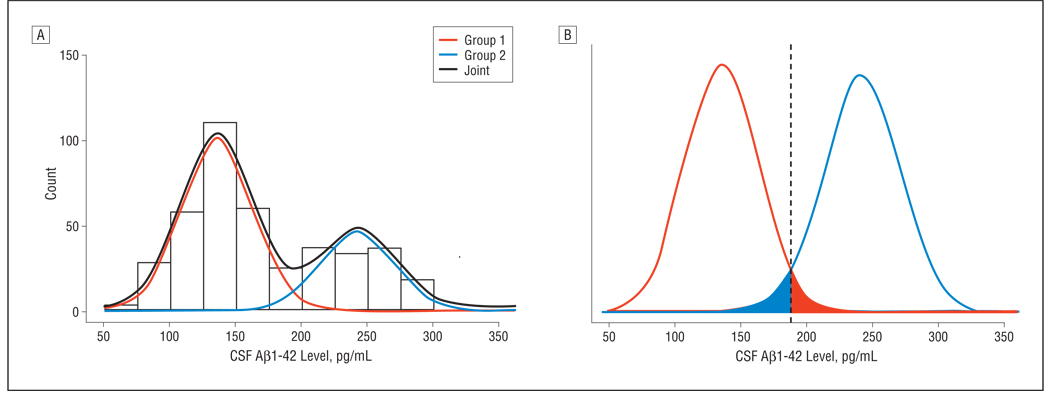
Design: Mixture modeling approach.
Setting: Alzheimer's Disease Neuroimaging Initiative database.
Patients or other participants: Cognitively normal persons, patients with AD, and individuals with mild cognitive impairment.
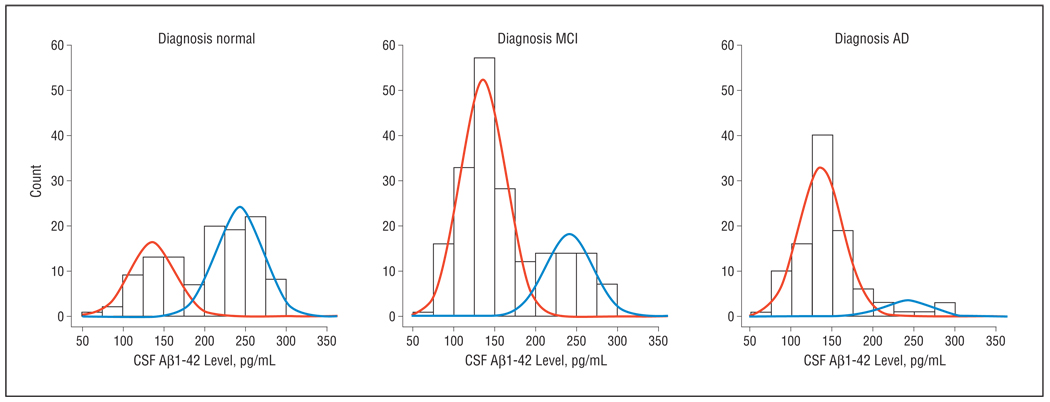
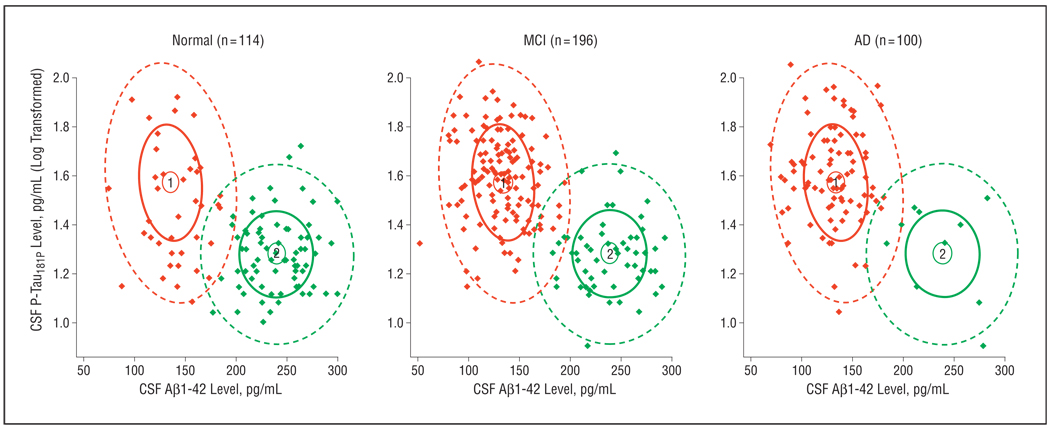
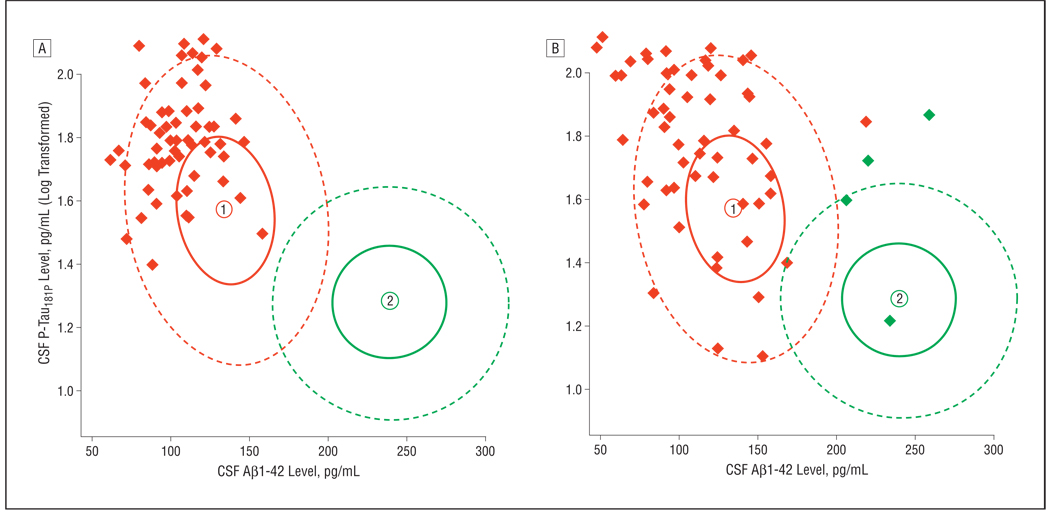
Main outcome measures: Cerebrospinal fluid-derived beta-amyloid protein 1-42, total tau protein, and phosphorylated tau(181P) protein concentrations were used as biomarkers on a clinically well-characterized data set. The outcome of the qualification analysis was validated on 2 additional data sets, 1 of which was autopsy confirmed.
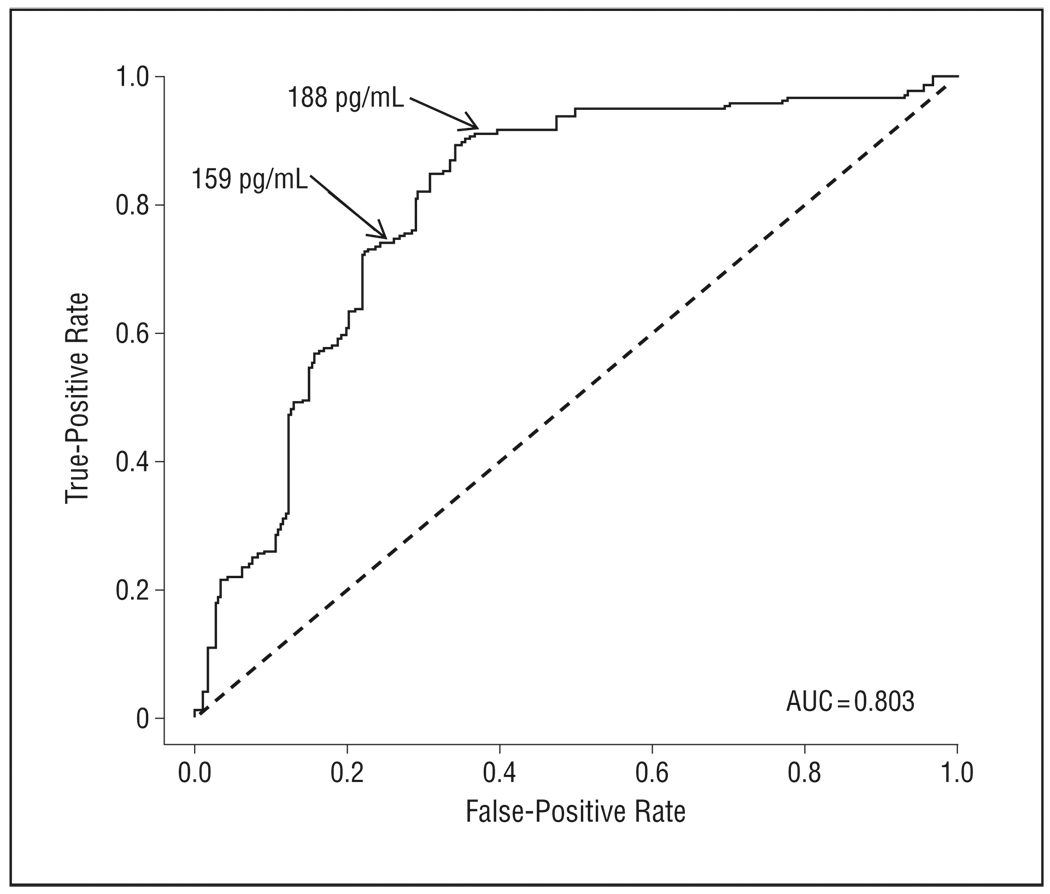
Results: Using the US Alzheimer's Disease Neuroimaging Initiative data set, a cerebrospinal fluid beta-amyloid protein 1-42/phosphorylated tau(181P) biomarker mixture model identified 1 feature linked to AD, while the other matched the "healthy" status. The AD signature was found in 90%, 72%, and 36% of patients in the AD, mild cognitive impairment, and cognitively normal groups, respectively. The cognitively normal group with the AD signature was enriched in apolipoprotein E epsilon4 allele carriers. Results were validated on 2 other data sets. In 1 study consisting of 68 autopsy-confirmed AD cases, 64 of 68 patients (94% sensitivity) were correctly classified with the AD feature. In another data set with patients (n = 57) with mild cognitive impairment followed up for 5 years, the model showed a sensitivity of 100% in patients progressing to AD.
Conclusions: The mixture modeling approach, totally independent of clinical AD diagnosis, correctly classified patients with AD. The unexpected presence of the AD signature in more than one-third of cognitively normal subjects suggests that AD pathology is active and detectable earlier than has heretofore been envisioned.
Figures
Comment in
-
Sharpen that needle.Arch Neurol. 2010 Aug;67(8):918-20. doi: 10.1001/archneurol.2010.151. Arch Neurol. 2010. PMID: 20697041 No abstract available.
-
The quest for biomarkers of Alzheimer's disease.J Am Geriatr Soc. 2011 Feb;59(2):377-8. doi: 10.1111/j.1532-5415.2011.03256.x. J Am Geriatr Soc. 2011. PMID: 21314665 No abstract available.
References
-
- Hansson O, Zetterberg H, Buchhave P, Londos E, Blennow K, Minthon L. Association between CSF biomarkers and incipient Alzheimer’s disease in patients with mild cognitive impairment: a follow-up study. Lancet Neurol. 2006;5(3):228–234. - PubMed
-
- Ray S, Britschgi M, Herbert C, et al. Classification and prediction of clinical Alzheimer’s diagnosis based on plasma signalling proteins. Nat Med. 2007;13(11):1359–1362. - PubMed
-
- Shaw LM, Korecka M, Clark CM, Lee VM, Trojanowski JQ. Biomarkers of neurodegeneration for diagnosis and monitoring therapeutics. Nat Rev Drug Discov. 2007;6(4):295–303. - PubMed
-
- Dubois B, Feldman HH, Jacova C, et al. Research criteria for the diagnosis of Alzheimer’s disease: revising the NINCDS-ADRDA criteria. Lancet Neurol. 2007;6(8):734–746. - PubMed
-
- Engelborghs S, De Vreese K, Van de Casteele T, et al. Diagnostic performance of a CSF-biomarker panel in autopsy-confirmed dementia. Neurobiol Aging. 2008;29:1143–1159. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
