

Tumor antigen-targeted, monoclonal antibody-based immunotherapy: clinical response, cellular immunity, and immunoescape
- PMID: 20697078
- PMCID: PMC2954137
- DOI: 10.1200/JCO.2009.27.6360
Tumor antigen-targeted, monoclonal antibody-based immunotherapy: clinical response, cellular immunity, and immunoescape
Abstract
Purpose: Tumor antigen (TA) -targeted monoclonal antibodies (mAb), rituximab, trastuzumab, and cetuximab, are clinically effective for some advanced malignancies, especially in conjunction with chemotherapy and/or radiotherapy. However, these results are only seen in a subset (20% to 30%) of patients. We discuss the immunologic mechanism(s) underlying these clinical findings and their potential role in the variability in patients' clinical response.
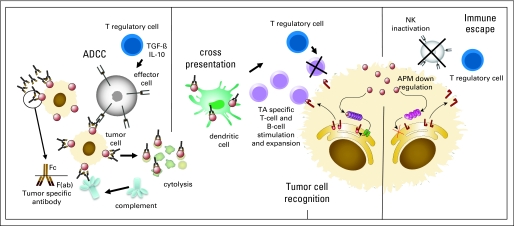
Methods: We reviewed the evidence indicating that the effects of TA-targeted mAb-based immunotherapy are mediated not only by inhibition of signaling pathways, but also by cell-mediated cytotoxicity triggered by the infused TA-targeted mAb. We analyzed the immunologic variables that can influence the outcome of antibody-dependent cell-mediated cytotoxicity (ADCC) in vitro and in animal model systems. We also analyzed the correlation reported between these variables and the clinical response to mAb-based immunotherapy.
Results: Of the variables that influence ADCC mediated by TA-targeted mAb, only polymorphisms of Fcγ receptors (FcγR) expressed by patients' lymphocytes were correlated with clinical efficacy. However, this correlation is not absolute and is not observed in all malignancies. Thus other variables may be responsible for the antitumor effects seen in mAb-treated patients. We discuss the evidence that triggering of TA-specific cellular immunity by TA-targeted mAb, in conjunction with immune escape mechanisms used by tumor cells, may contribute to the differential clinical responses to mAb-based immunotherapy.
Conclusion: Identification of the mechanism(s) underlying the clinical response of patients with cancer treated with TA-targeted mAb is crucial to optimizing their application in the clinic and to selecting the patients most likely to benefit from their use.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Musolino A, Naldi N, Bortesi B, et al. Immunoglobulin G fragment C receptor polymorphisms and clinical efficacy of trastuzumab-based therapy in patients with HER-2/neu-positive metastatic breast cancer. J Clin Oncol. 2008;26:1789–1796. - PubMed
-
- Weng WK, Czerwinski D, Timmerman J, et al. Clinical outcome of lymphoma patients after idiotype vaccination is correlated with humoral immune response and immunoglobulin G Fc receptor genotype. J Clin Oncol. 2004;22:4717–4724. - PubMed
-
- Weng WK, Levy R. Two immunoglobulin G fragment C receptor polymorphisms independently predict response to rituximab in patients with follicular lymphoma. J Clin Oncol. 2003;21:3940–3947. - PubMed
-
- Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. 2006;354:567–578. - PubMed
-
- Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008;359:1116–1127. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
