

Recurrent ovarian cancer: use of contrast-enhanced CT and PET/CT to accurately localize tumor recurrence and to predict patients' survival
- PMID: 20697116
- PMCID: PMC3726307
- DOI: 10.1148/radiol.10092279
Recurrent ovarian cancer: use of contrast-enhanced CT and PET/CT to accurately localize tumor recurrence and to predict patients' survival
Abstract
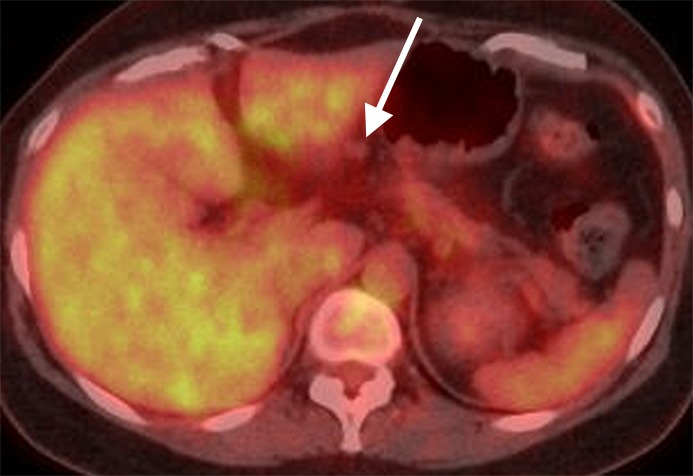
Purpose: To compare accuracy and interobserver variability in the detection and localization of recurrent ovarian cancer with contrast material-enhanced (CE) computed tomography (CT) and positron emission tomography (PET)/CT and determine whether imaging findings can be used to predict survival.
Materials and methods: Waiving informed consent, the institutional review board approved this HIPAA-compliant, retrospective study of 35 women (median age, 54.4 years) with histopathologically proven recurrent ovarian carcinoma who underwent CE CT and PET/CT before exploratory surgery. All CE CT and PET/CT scans were independently analyzed. Tumor presence, number of lesions, and the size and maximum standardized uptake value (SUV(max)) of the largest lesion were recorded for patient and region. Surgical histopathologic findings constituted the reference standard. Areas under the receiver operating characteristic curves (AUCs), κ statistics, and hazard ratios were calculated.
Results: Readers' AUCs in detection of recurrence for region were 0.85 (95% confidence interval [CI]: 0.81, 0.90) and 0.78 (95% CI: 0.72, 0.83) for CE CT and 0.84 (95% CI: 0.79, 0.89) and 0.74 (95% CI: 0.67, 0.81) for PET/CT (P = .76); 12 patients died. At PET/CT, size, number, and SUV(max) of peritoneal deposits were significantly associated with poor survival for readers 1 and 2 (P ≤ .01and ≤ .05, respectively), as were long- and short-axis diameters, number, and SUV(max) of distant lymph nodes for reader 1 (P ≤ .001). With CE CT, size (reader 1) and number (readers 1 and 3) of peritoneal deposits were significantly associated with poor survival (P ≤ .01), as were long- and short-axis diameters and number of distant lymph nodes for reader 1 (P ≤ .01). Interobserver agreement ranged from fair (patient, κ = 0.30) to moderate (region, κ = 0.55) for CE CT and fair (patient, κ = 0.24) to substantial (region, κ = 0.63) for PET/CT.
Conclusion: Preliminary data suggest that CE CT and PET/CT may have similar accuracy in detection of recurrent ovarian cancer. Tumor size, number, and SUV(max) may have potential as prognostic biomarkers for patients with recurrent ovarian cancer.
Conflict of interest statement
Authors stated no financial relationship to disclose.
Figures





References
-
- American Cancer Society Cancer facts & figures 2009. Atlanta, Ga: American Cancer Society, 2009
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin 2009;59(4):225–249 - PubMed
-
- Omura GA, Brady MF, Homesley HD, et al. Long-term follow-up and prognostic factor analysis in advanced ovarian carcinoma: the Gynecologic Oncology Group experience. J Clin Oncol 1991;9(7):1138–1150 - PubMed
-
- Rose PG. Surgery for recurrent ovarian cancer. Semin Oncol 2000;27(3 suppl 7):17–23 - PubMed
-
- Folk JJ, Botsford M, Musa AG. Monitoring cancer antigen 125 levels in induction chemotherapy for epithelial ovarian carcinoma and predicting outcome of second-look procedure. Gynecol Oncol 1995;57(2):178–182 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
