

Quantitative analysis of cell composition and purity of human pancreatic islet preparations
- PMID: 20697378
- PMCID: PMC2966538
- DOI: 10.1038/labinvest.2010.124
Quantitative analysis of cell composition and purity of human pancreatic islet preparations
Abstract
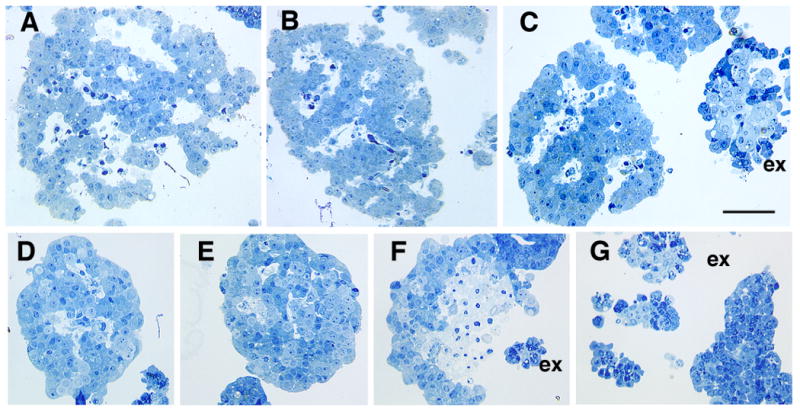
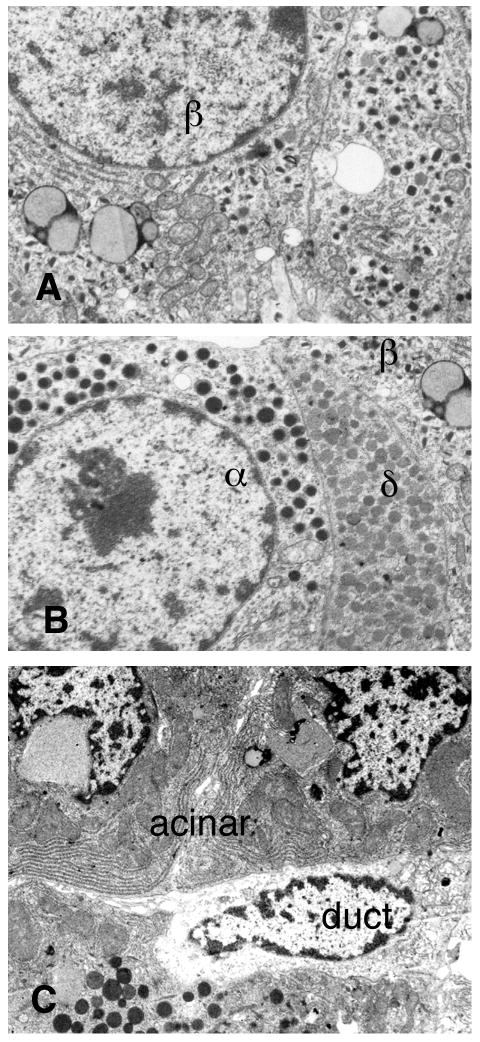
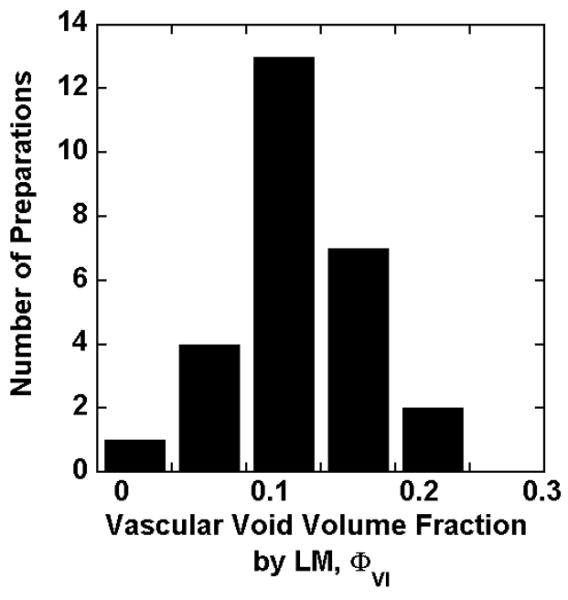
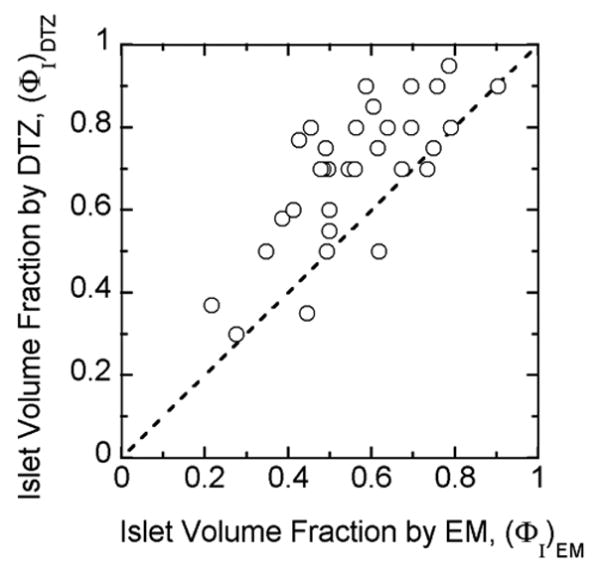
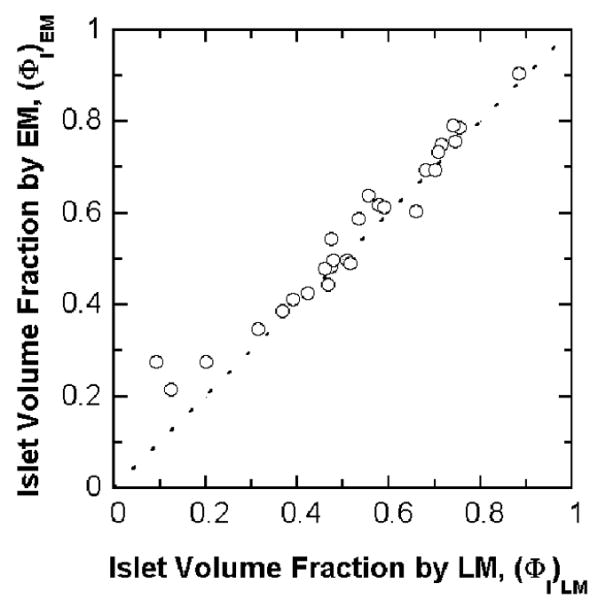
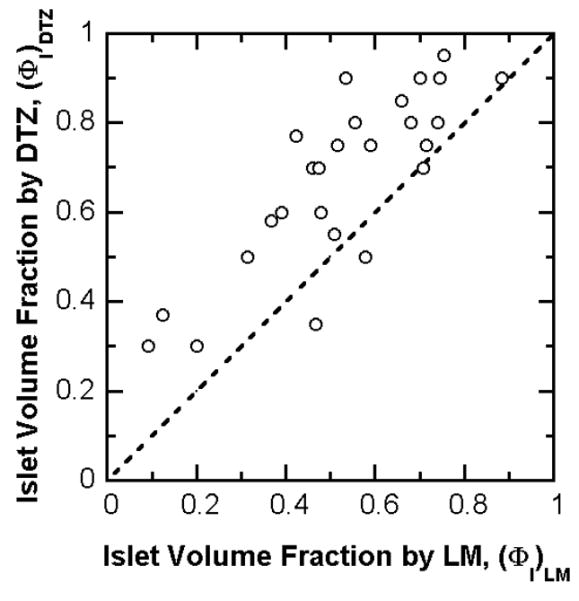
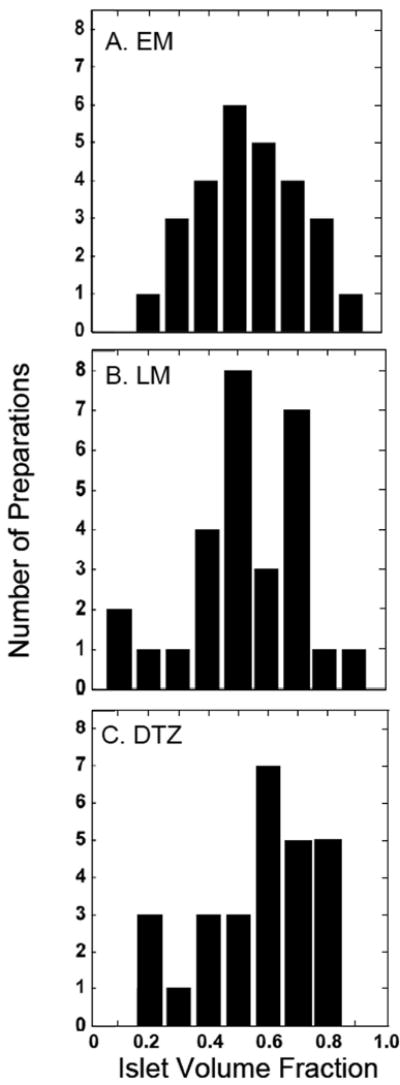
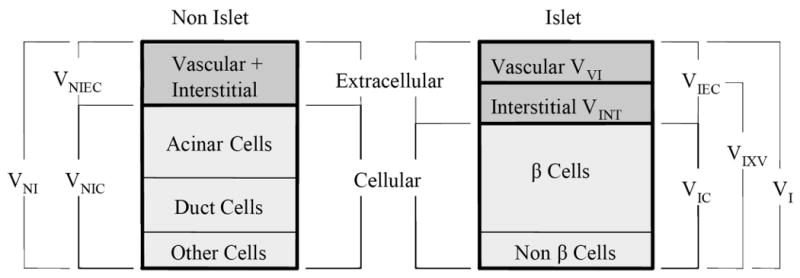
Despite improvements in outcomes for human islet transplantation, characterization of islet preparations remains poorly defined. This study used both light microscopy (LM) and electron microscopy (EM) to characterize 33 islet preparations used for clinical transplants. EM allowed an accurate identification and quantification of cell types with measured cell number fractions (mean±s.e.m.) of 35.6±2.1% β-cells, 12.6±1.0% non-β-islet cells (48.3±2.6% total islet cells), 22.7±1.5% duct cells, and 25.3±1.8% acinar cells. Of the islet cells, 73.6±1.7% were β-cells. For comparison with the literature, estimates of cell number fraction, cell volume, and extracellular volume were combined to convert number fraction data to volume fractions applicable to cells, islets, and the entire preparation. The mathematical framework for this conversion was developed. By volume, β-cells were 86.5±1.1% of the total islet cell volume and 61.2±0.8% of intact islets (including the extracellular volume), which is similar to that of islets in the pancreas. Our estimates produced 1560±20 cells in an islet equivalent (volume of 150-μm diameter sphere), of which 1140±15 were β-cells. To test whether LM analysis of the same tissue samples could provide reasonable estimates of purity of the islet preparations, volume fraction of the islet tissue was measured on thin sections available from 27 of the clinical preparations by point counting morphometrics. Islet purity (islet volume fraction) of individual preparations determined by LM and EM analyses correlated linearly with excellent agreement (R²=0.95). However, islet purity by conventional dithizone staining was substantially higher with a 20-30% overestimation. Thus, both EM and LM provide accurate methods to determine the cell composition of human islet preparations and can help us understand many of the discrepancies of islet composition in the literature.
Conflict of interest statement
Figures
References
-
- Hering BJ, Kandaswamy R, Ansite JD, Eckman PM, Nakano M, Sawada T, et al. Single-donor, marginal-dose islet transplantation in patients with type 1 diabetes. JAMA. 2005;293:830–5. - PubMed
-
- Ryan EA, Paty BW, Senior PA, Bigam D, Alfadhli E, Kneteman NM, et al. Five-year follow-up after clinical islet transplantation. Diabetes. 2005;54:2060–9. - PubMed
-
- Street CN, Lakey JR, Shapiro AM, Imes S, Rajotte RV, Ryan EA, et al. Islet graft assessment in the Edmonton Protocol: implications for predicting long-term clinical outcome. Diabetes. 2004;53:3107–14. - PubMed
-
- Goto M, Eich TM, Felldin M, Foss A, Kallen R, Salmela K, et al. Refinement of the automated method for human islet isolation and presentation of a closed system for in vitro islet culture. Transplantation. 2004;78:1367–75. - PubMed
-
- Keymeulen B, Ling Z, Gorus FK, Delvaux G, Bouwens L, Grupping A, et al. Implantation of standardized beta-cell grafts in a liver segment of IDDM patients: graft and recipient characteristics in two cases of insulin-independence under maintenance immunosuppression for prior kidney graft. Diabetologia. 1998;41:452–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
