

Surgery in the patient with liver disease
- PMID: 20697561
- PMCID: PMC2917124
Surgery in the patient with liver disease
Abstract
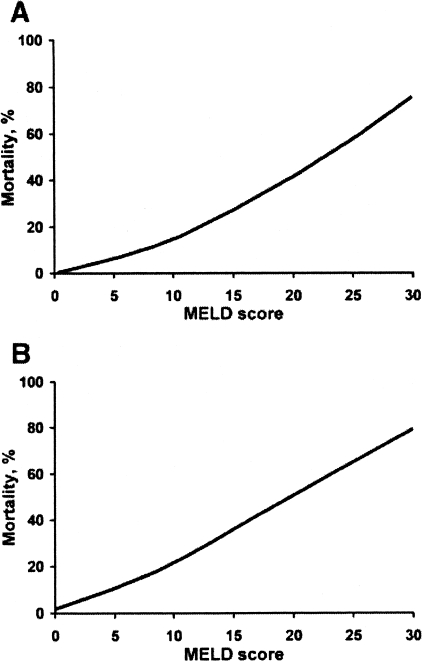
Surgery is performed in patients with liver disease more frequently now than in the past, in part because of the long-term survival of patients with cirrhosis. Recent work has focused on estimating perioperative risk in patients with liver disease. Hemodynamic instability in the perioperative period can worsen liver function in patients with liver disease. Operative risk correlates with the severity of the underlying liver disease and the nature of the surgical procedure. Thorough preoperative evaluation is necessary prior to elective surgery. Surgery is contraindicated in patients with certain conditions, such as acute hepatitis, acute liver failure, and alcoholic hepatitis. Estimation of perioperative mortality is inexact because of the retrospective nature of and biased patient selection in available clinical studies. The Child-Pugh classification (Child-Turcotte-Pugh score) and particulary the Model for End-Stage Liver Disease (MELD) score provide reasonable estimations of perioperative mortality but do not replace the need for careful preoperative preparation and postoperative monitoring, as early detection of complications is essential for improving outcomes. Medical therapy for specific manifestations of hepatic disease, including ascites, encephalopathy, and renal dysfunction, should be optimized preoperatively or, if necessary, administered in the postoperative period.
Conflict of interest statement
Potential Conflicts of Interest: None disclosed.
Figures
References
-
- Friedman LS. The risk of surgery in patients with liver disease. Hepatology. 1999;29:1617–23. - PubMed
-
- Gholson CF, Provenza JM, Bacon BR. Hepatologic considerations in patients with parenchymal liver disease undergoing surgery. Am J Gastroenterol. 1990;85:487–96. - PubMed
-
- Gelman S. General anesthesia and hepatic circulation. Can J Physiol Pharmacol. 1987;65:1762–79. - PubMed
-
- Sato K, Kawamura T, Wakusawa R. Hepatic blood flow and function in elderly patients undergoing laparoscopic cholecystectomy. Anesth Analg. 2000;90:1198–202. - PubMed
-
- Lai HC, Wang KY, Lee WL, et al. Severe pulmonary hypertension complicates postoperative outcome of non-cardiac surgery. Br J Anaesth. 2007;99:184–90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous