

Supratentorial glioblastoma multiforme: the role of surgical resection versus biopsy among older patients
- PMID: 20697823
- PMCID: PMC4612568
- DOI: 10.1245/s10434-010-1242-6
Supratentorial glioblastoma multiforme: the role of surgical resection versus biopsy among older patients
Abstract
Background: The peak incidence of glioblastoma multiforme (GBM) occurs in those aged 65 years and older. However, studies on this patient group remain limited. The goal of this study is to evaluate the efficacy of surgery versus biopsy for older patients with these lesions.
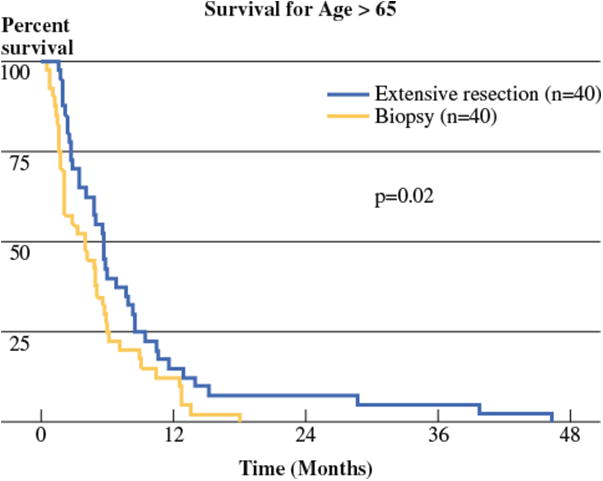
Methods: 133 and 72 consecutive patients aged 65 years and older who underwent surgery and needle biopsy for intracranial primary (de novo) GBM between 1997 and 2007 were retrospectively reviewed. Among these patients, 40 who underwent surgical resection were matched with 40 who underwent needle biopsy alone for factors consistently shown to be associated with survival [age, Karnofsky Performance Scale (KPS) indexing, eloquent involvement, radiation, temozolomide]. Survival was expressed as estimated Kaplan-Meier plots, and log-rank analysis was used to compare survival curves.
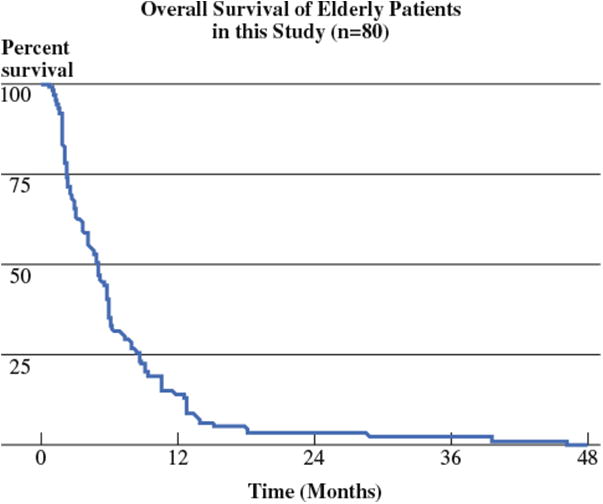
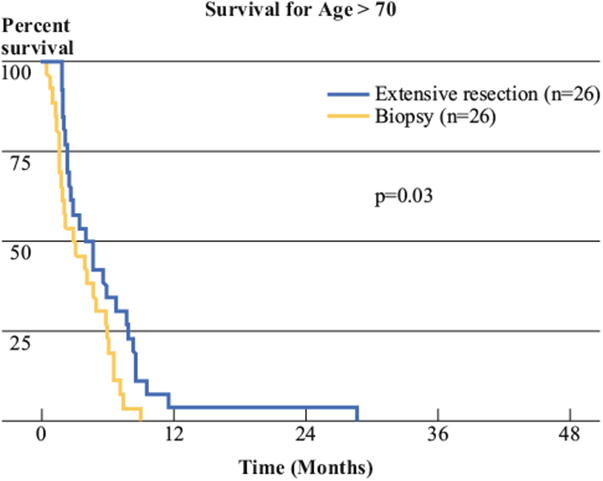
Results: Mean ± standard deviation age was 73 ± 5 years, and median survival was 4.9 months. There were no significant differences in perioperative outcomes among patients who underwent surgical resection versus needle biopsy. Patients who underwent resection had median survival of 5.7 months as compared with 4.0 months for patients who underwent needle biopsy (P = 0.02). Likewise, for patients aged 70 years and older, median survival was 4.5 months for 26 patients who underwent surgical resection as compared with 3.0 months for 26 patients who underwent needle biopsy (P = 0.03).
Conclusion: This study demonstrates that older patients tolerate aggressive surgery without increased surgery-related morbidity and have prolonged survival as compared with similar patients undergoing needle biopsy. These findings may help guide treatment decisions for patients, their families, and their physicians.
Figures
References
-
- Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;10:997–1003. - PubMed
-
- Barnholtz-Sloan JS, Williams VL, Maldonado JL, Shahani D, Stockwell HG, Chamberlain M, et al. Patterns of care and outcomes among elderly individuals with primary malignant astrocytoma. J Neurosurg. 2008;4:642–8. - PubMed
-
- Brem H, Piantadosi S, Burger PC, Walker M, Selker R, Vick NA, et al. Placebo-controlled trial of safety and efficacy of intraoperative controlled delivery by biodegradable polymers of chemotherapy for recurrent gliomas. The Polymer-brain Tumor Treatment Group. Lancet. 1995;8956:1008–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
