

Ability among adolescents for the metabolic syndrome to predict elevations in factors associated with type 2 diabetes and cardiovascular disease: data from the national health and nutrition examination survey 1999-2006
- PMID: 20698802
- PMCID: PMC3046372
- DOI: 10.1089/met.2010.0008
Ability among adolescents for the metabolic syndrome to predict elevations in factors associated with type 2 diabetes and cardiovascular disease: data from the national health and nutrition examination survey 1999-2006
Abstract
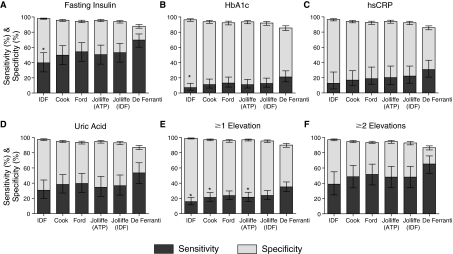
Objective: The aim of this study was to compare currently proposed sets of pediatric metabolic syndrome criteria for the ability to predict elevations in "surrogate" factors that are associated with metabolic syndrome and with future cardiovascular disease and type 2 diabetes mellitus. These surrogate factors were fasting insulin, hemoglobin A1c (HbA1c), high-sensitivity C-reactive protein (hsCRP), and uric acid.
Methods: Waist circumference (WC), blood pressure, triglycerides, high-density lipoprotein cholesterol (HDL-C), fasting glucose, fasting insulin, HbA1c, hsCRP, and uric acid measurements were obtained from 2,624 adolescent (12-18 years old) participants of the 1999-2006 National Health and Nutrition Examination Surveys. We identified children with metabolic syndrome as defined by six commonly used sets of pediatric metabolic syndrome criteria. We then defined elevations in the surrogate factors as values in the top 5% for the cohort and calculated sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for each set of metabolic syndrome criteria and for each surrogate factor.
Results: Current pediatric metabolic syndrome criteria exhibited variable sensitivity and specificity for surrogate predictions. Metabolic syndrome criteria had the highest sensitivity for predicting fasting insulin (40-70%), followed by uric acid (31-54%), hsCRP (13-31%), and HbA1c (7-21%). The criteria of de Ferranti (which includes children with WC >75(th) percentile, compared to all other sets including children with WC >90(th) percentile) exhibited the highest sensitivity for predicting each of the surrogates, with only modest decrease in specificity compared to the other sets of criteria. However, the de Ferranti criteria also exhibited the lowest PPV values. Conversely, the pediatric International Diabetes Federation criteria exhibited the lowest sensitivity and the highest specificity.
Conclusions: Pediatric metabolic syndrome criteria exhibit moderate sensitivity for detecting elevations in surrogate factors associated with metabolic syndrome and with risk for future disease. Inclusion of children with more modestly elevated WC improved sensitivity.
Figures
References
-
- Narayan KM. Boyle JP. Thompson TJ. Sorensen SW. Williamson DF. Lifetime risk for diabetes mellitus in the United States. JAMA. 2003;290:1884–1890. - PubMed
-
- Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37:1595–1607. - PubMed
-
- Haffner SM. The metabolic syndrome: Inflammation, diabetes mellitus, and cardiovascular disease. Am J Cardiol. 2006;97:3A–11A. - PubMed
-
- Morrison JA. Friedman LA. Wang P. Glueck CJ. Metabolic syndrome in childhood predicts adult metabolic syndrome and type 2 diabetes mellitus 25 to 30 years later. J Pediatr. 2008;152:201–206. - PubMed
-
- Zimmet P. Alberti G. Kaufman F. Tajima N. Silink M. Arslanian S. Wong G. Bennett P. Shaw J. Caprio S. International Diabetes Federation Task Force on Epidemiology Prevention of Diabetes. The metabolic syndrome in children and adolescents. Lancet. 2007;369:2059–2061. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials