

Medicare payments for common inpatient procedures: implications for episode-based payment bundling
- PMID: 20698899
- PMCID: PMC3026958
- DOI: 10.1111/j.1475-6773.2010.01150.x
Medicare payments for common inpatient procedures: implications for episode-based payment bundling
Abstract
Background: Aiming to align provider incentives toward improving quality and efficiency, the Center for Medicare and Medicaid Services is considering broader bundling of hospital and physician payments around episodes of inpatient surgery. Decisions about bundled payments would benefit from better information about how payments are currently distributed among providers of different perioperative services and how payments vary across hospitals.
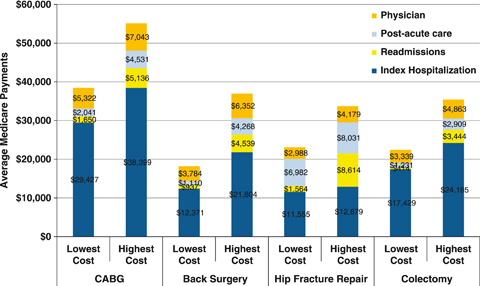
Study design: Using the national Medicare database, we identified patients undergoing one of four inpatient procedures in 2005 (coronary artery bypass [CABG], hip fracture repair, back surgery, and colectomy). For each procedure, price-standardized Medicare payments from the date of admission for the index procedure to 30 days postdischarge were assessed and categorized by payment type (hospital, physician, and postacute care) and subtype.
Results: Average total payments for inpatient surgery episodes varied from U.S.$26,515 for back surgery to U.S.$45,358 for CABG. Hospital payments accounted for the largest share of total payments (60-80 percent, depending on procedure), followed by physician payments (13-19 percent) and postacute care (7-27 percent). Overall episode payments for hospitals in the lowest and highest payment quartiles differed by U.S.$16,668 for CABG, U.S.$18,762 for back surgery, U.S.$10,615 for hip fracture repair, and U.S.$12,988 for colectomy. Payments to hospitals accounted for the largest share of variation in payments. Among specific types of payments, those associated with 30-day readmissions and postacute care varied most substantially across hospitals.
Conclusions: Fully bundled payments for inpatient surgical episodes would need to be dispersed among many different types of providers. Hospital payments--both overall and for specific services--vary considerably and might be reduced by incentives for hospitals and physicians to improve quality and efficiency.
© Health Research and Educational Trust.
Figures
References
-
- Abelson R. “In Bid for Better Care, Surgery with a Warranty.”New York Times 2007: A1.
-
- Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction. Journal of American Medical Association. 2002;288(16):1987–93. - PubMed
-
- Dimick JB, Weeks WB, Karia RJ, Das S, Campbell DAJ. Who Pays for Poor Surgical Quality? Building a Business Case for Quality Improvement. Journal of the American College of Surgeons. 2006;202:933–7. - PubMed
-
- Gottlieb DJ, Zhou W, Sung Y, Sutherland JM, Andrews K, Skinner JS. Adjusting Medicare Expenditures for Regional Differences in Prices. Medical Care. 2010 (in press)
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
