

Haemodynamic optimisation improves tissue microvascular flow and oxygenation after major surgery: a randomised controlled trial
- PMID: 20698956
- PMCID: PMC2945135
- DOI: 10.1186/cc9220
Haemodynamic optimisation improves tissue microvascular flow and oxygenation after major surgery: a randomised controlled trial
Abstract
Introduction: Post-operative outcomes may be improved by the use of flow related end-points for intra-venous fluid and/or low dose inotropic therapy. The mechanisms underlying this benefit remain uncertain. The objective of this study was to assess the effects of stroke volume guided intra-venous fluid and low dose dopexamine on tissue microvascular flow and oxygenation and inflammatory markers in patients undergoing major gastrointestinal surgery.
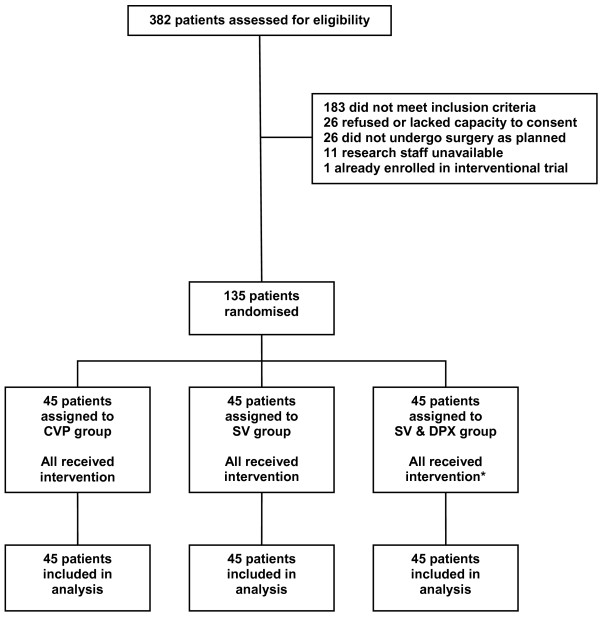
Methods: Randomised, controlled, single blind study of patients admitted to a university hospital critical care unit following major gastrointestinal surgery. For eight hours after surgery, intra-venous fluid therapy was guided by measurements of central venous pressure (CVP group), or stroke volume (SV group). In a third group stroke volume guided fluid therapy was combined with dopexamine (0.5 mcg/kg/min) (SV & DPX group).
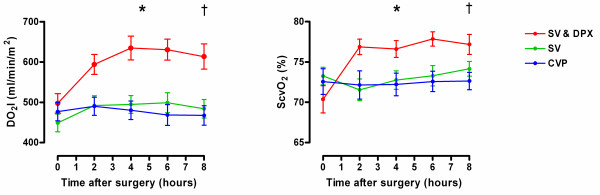
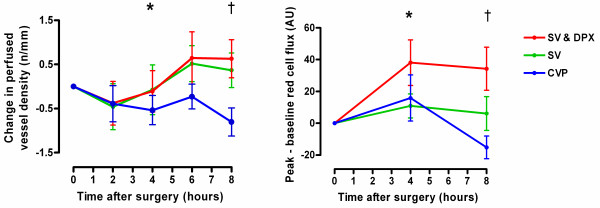
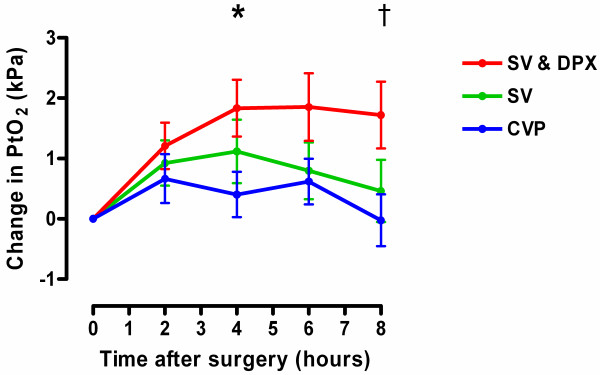
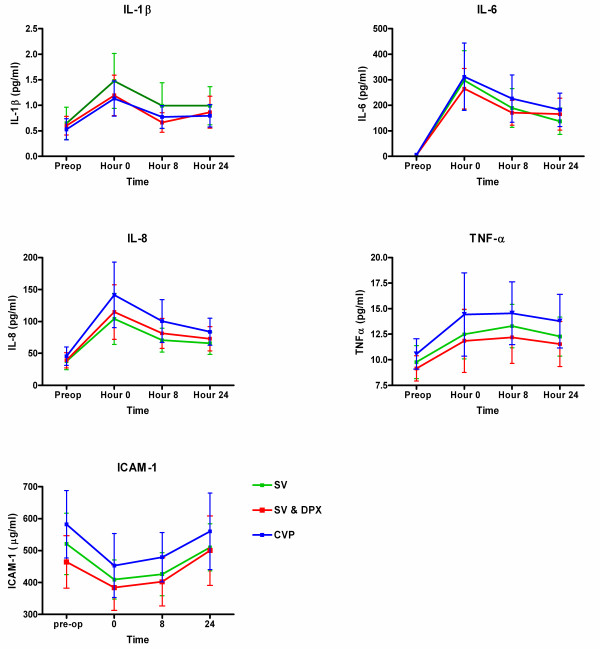
Results: 135 patients were recruited (n = 45 per group). In the SV & DPX group, increased global oxygen delivery was associated with improved sublingual (P < 0.05) and cutaneous microvascular flow (P < 0.005) (sublingual microscopy and laser Doppler flowmetry). Microvascular flow remained constant in the SV group but deteriorated in the CVP group (P < 0.05). Cutaneous tissue oxygen partial pressure (PtO2) (Clark electrode) improved only in the SV & DPX group (P < 0.001). There were no differences in serum inflammatory markers. There were no differences in overall complication rates between the groups although acute kidney injury was more frequent in the CVP group (CVP group ten patients (22%); pooled SV and SV & DPX groups seven patients (8%); P = 0.03) (post hoc analysis).
Conclusions: Stroke volume guided fluid and low dose inotropic therapy was associated with improved global oxygen delivery, microvascular flow and tissue oxygenation but no differences in the inflammatory response to surgery. These observations may explain improved clinical outcomes associated with this treatment in previous trials.
Trial registration number: ISRCTN 94850719.
Figures
Comment in
-
Inotropes in goal-directed therapy: do we need 'goals'?Crit Care. 2010;14(5):1001. doi: 10.1186/cc9251. Epub 2010 Sep 29. Crit Care. 2010. PMID: 20920151 Free PMC article.
References
-
- Cullinane M, Gray AJ, Hargraves CM, Lansdown M, Martin IC, Schubert M. The 2003 Report of the National Confidential Enquiry into Peri-Operative Deaths. London: NCEPOD; 2003.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
