

Fluoroscopically guided transforaminal epidural dry needling for lumbar spinal stenosis using a specially designed needle
- PMID: 20698999
- PMCID: PMC2927508
- DOI: 10.1186/1471-2474-11-180
Fluoroscopically guided transforaminal epidural dry needling for lumbar spinal stenosis using a specially designed needle
Abstract
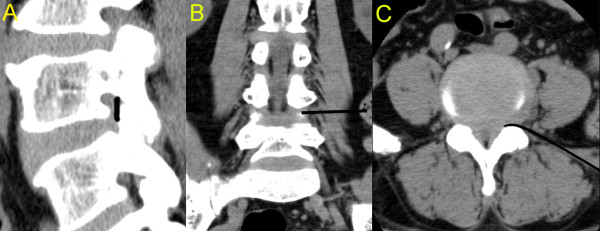
Background: This report describes the methodological approach and clinical application of a minimally invasive intervention to treat lumbar spinal stenosis (LSS).
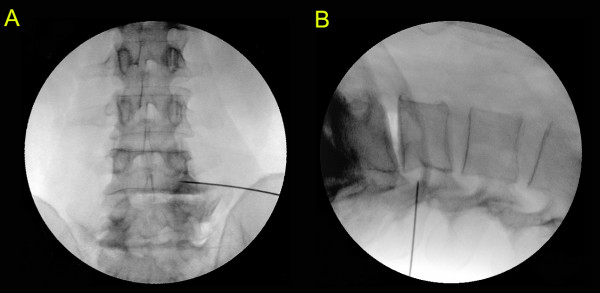
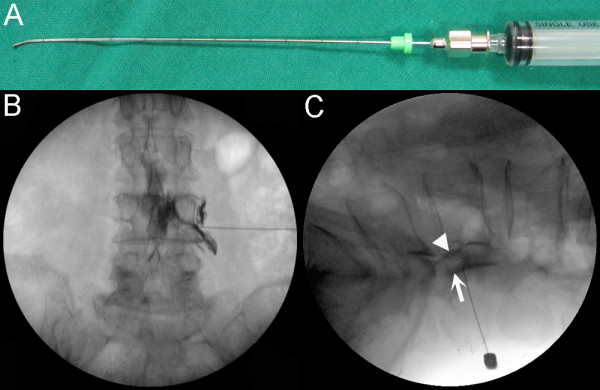
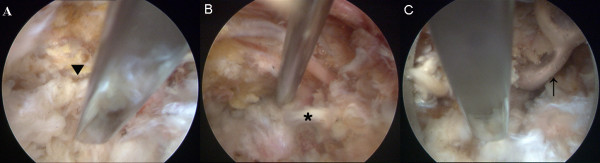
Methods: Thirty-four patients with LSS underwent fluoroscopically guided transforaminal epidural dry needling using a specially designed flexed Round Needle. The needle was inserted 8-12 cm lateral to the midline at the level of the stenosis and advanced to a position between the anterior side of the facet joint and pedicle up to the outer-third of the pedicle. The needle was advanced medially and backed laterally within a few millimetres along the canal side of the inferior articular process between the facet joint and pedicle. The procedure was completed when a marked reduction in resistance was felt at the tip of the needle. The procedure was performed bilaterally at the level of the stenosis.
Results: The average follow-up period was 12.9 +/- 1.1 months. The visual analogue scale (VAS) pain score was reduced from 7.3 +/- 2.0 to 4.6 +/- 2.5 points, the Oswestry Disability Index (ODI) score decreased from 41.4 +/- 17.2 to 25.5 +/- 12.6% and the average self-rated improvement was 52.6 +/- 33.1%. The VAS scores indicated that 14 (41.2%) patients reported a "good" to "excellent" treatment response, while 11 (32.4%) had a "good" to "excellent" treatment response on the ODI and 22 (64.7%) had a "good" to "excellent" treatment response on the self-rated improvement scale.
Conclusions: These results suggest that fluoroscopically guided transforaminal epidural dry needling is effective for managing LSS.
Figures

References
-
- Weinstein PR. Diagnosis and management of lumbar spinal stenosis. Clin Neurosurg. 1983;30:677–697. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
