

Renal cancer resistance to antiangiogenic therapy is delayed by restoration of angiostatic signaling
- PMID: 20699227
- PMCID: PMC2956167
- DOI: 10.1158/1535-7163.MCT-10-0477
Renal cancer resistance to antiangiogenic therapy is delayed by restoration of angiostatic signaling
Abstract
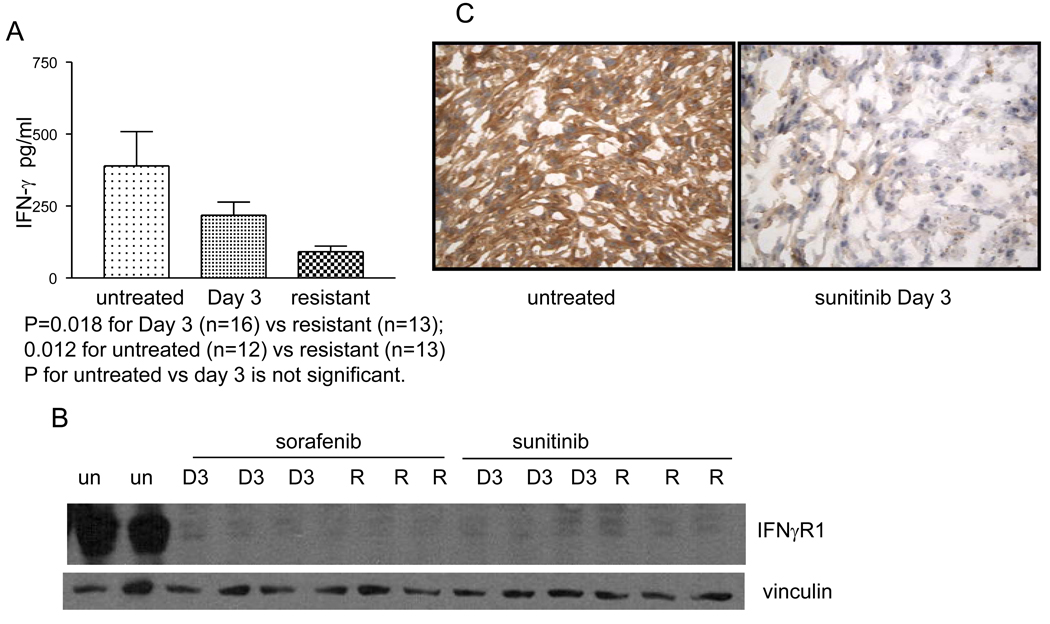
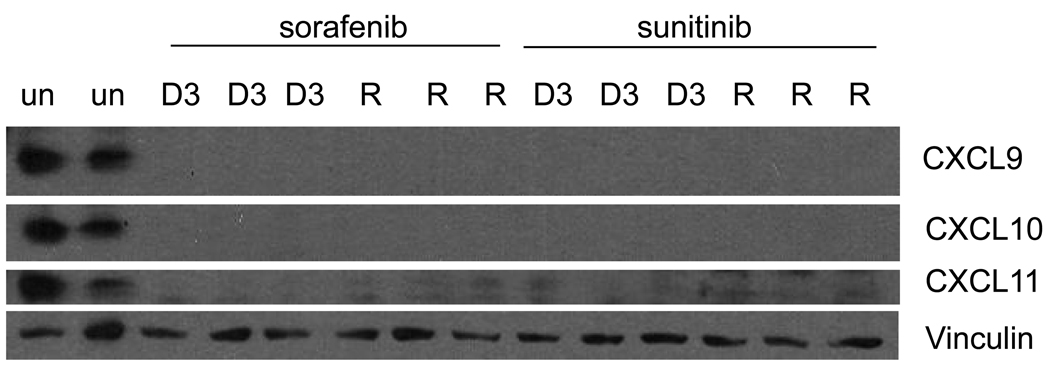
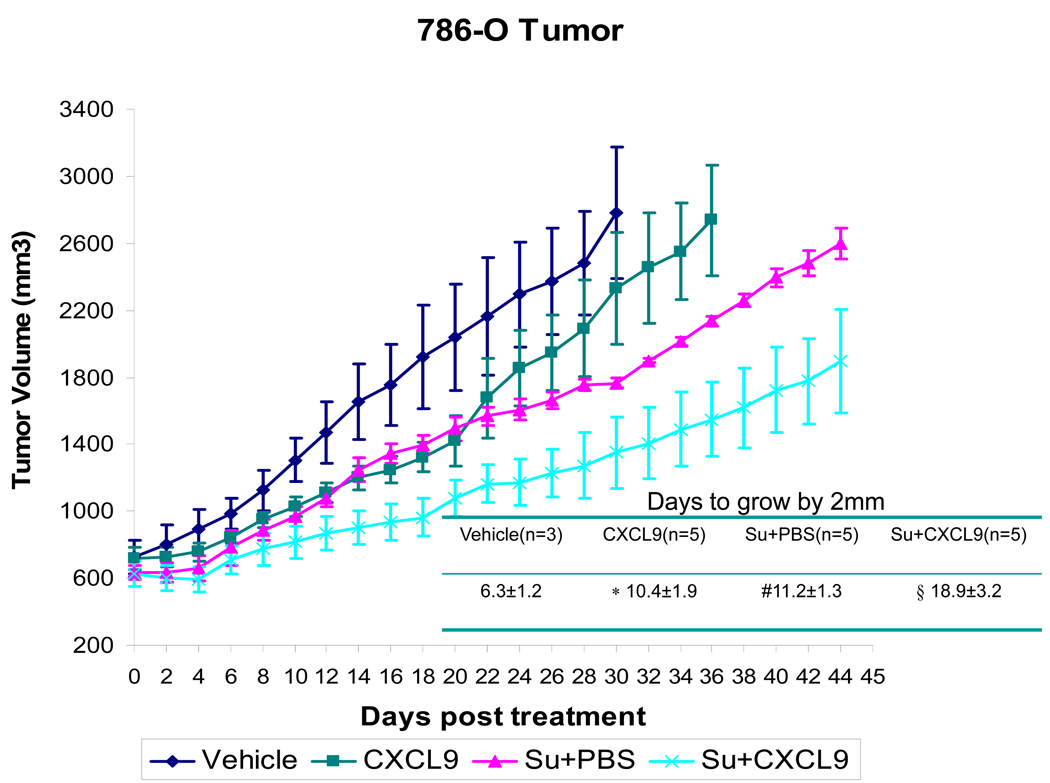
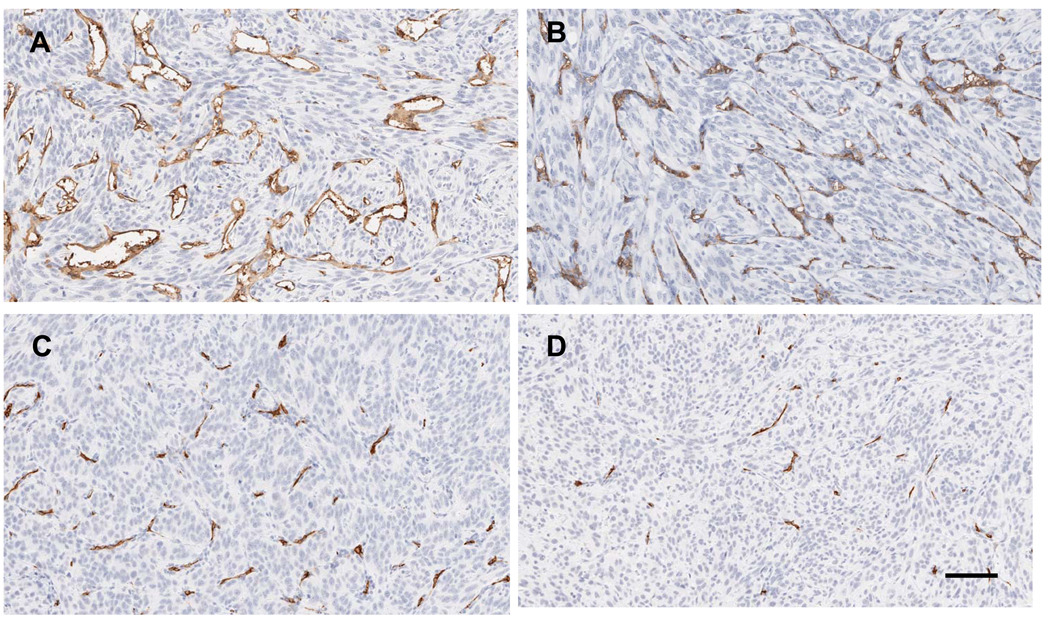
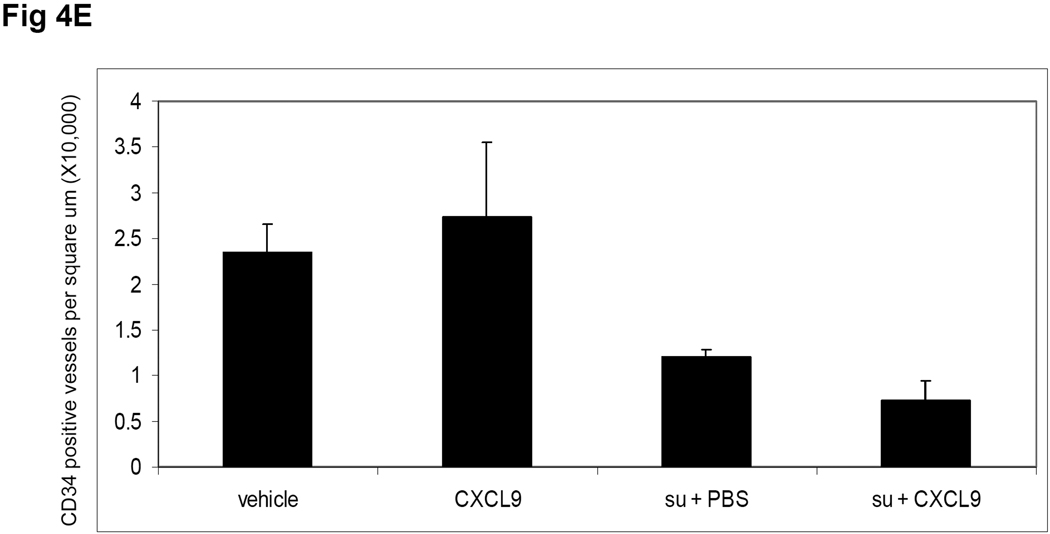
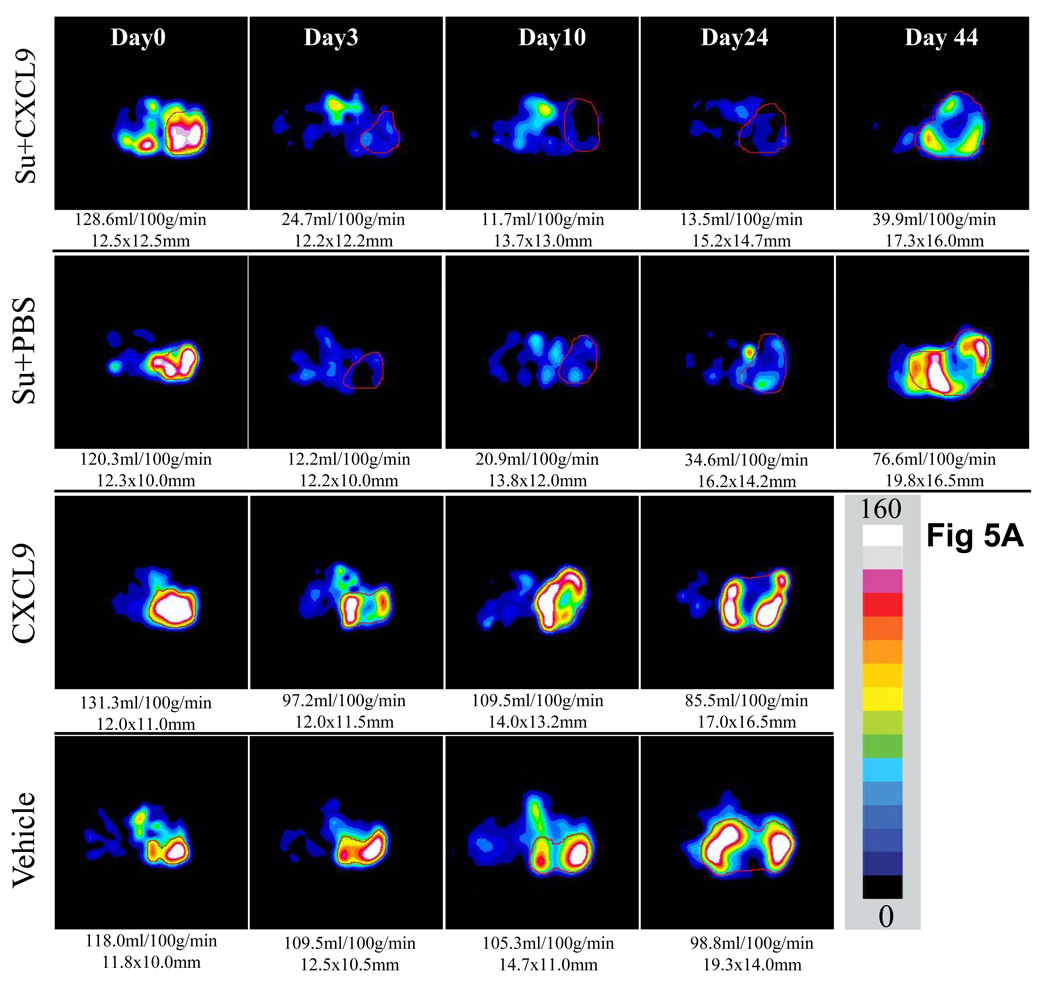
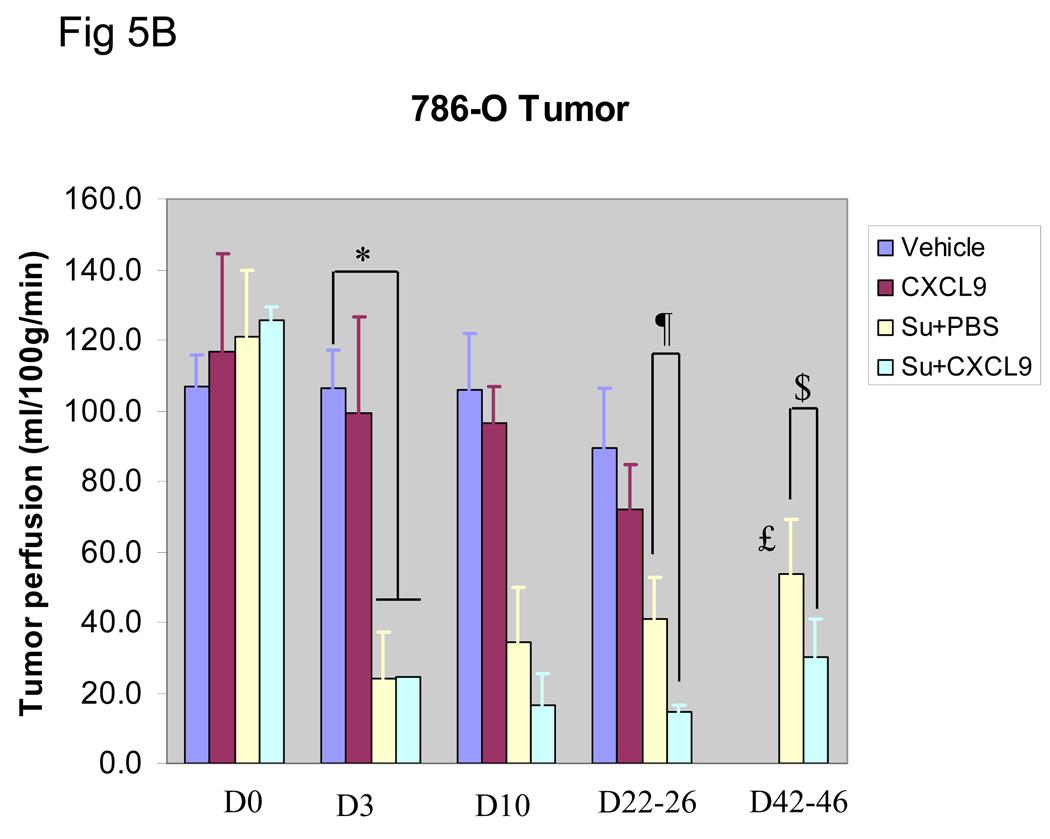
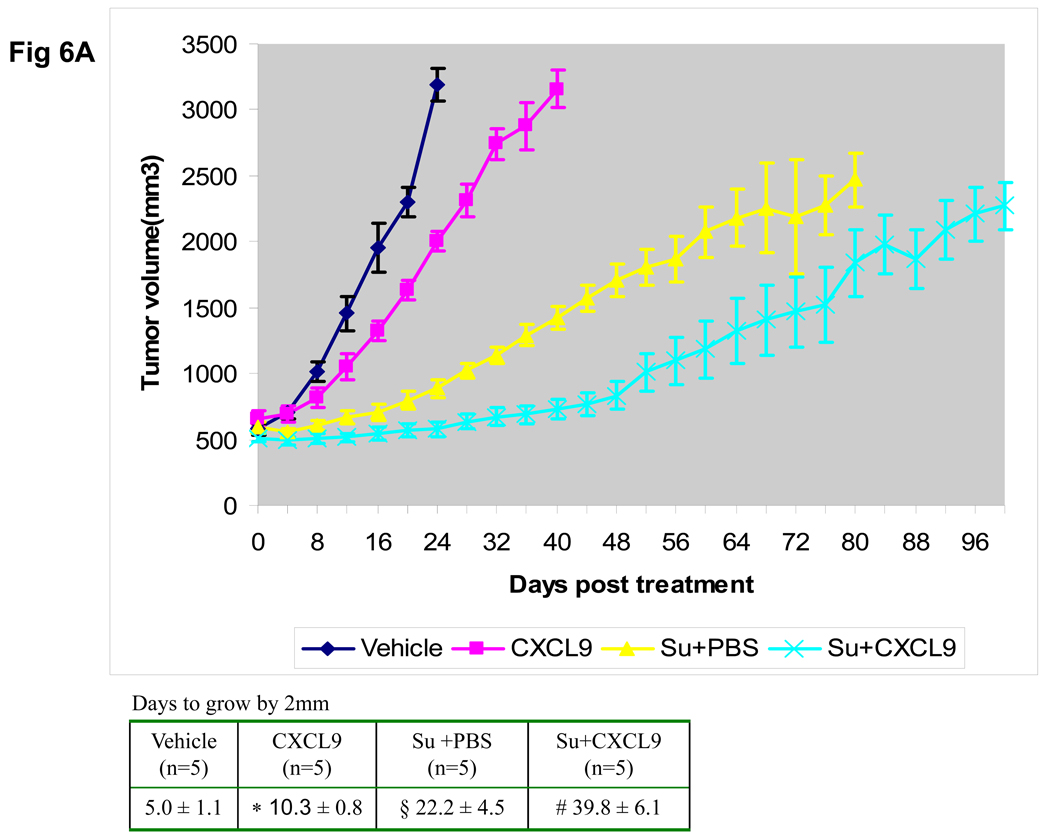
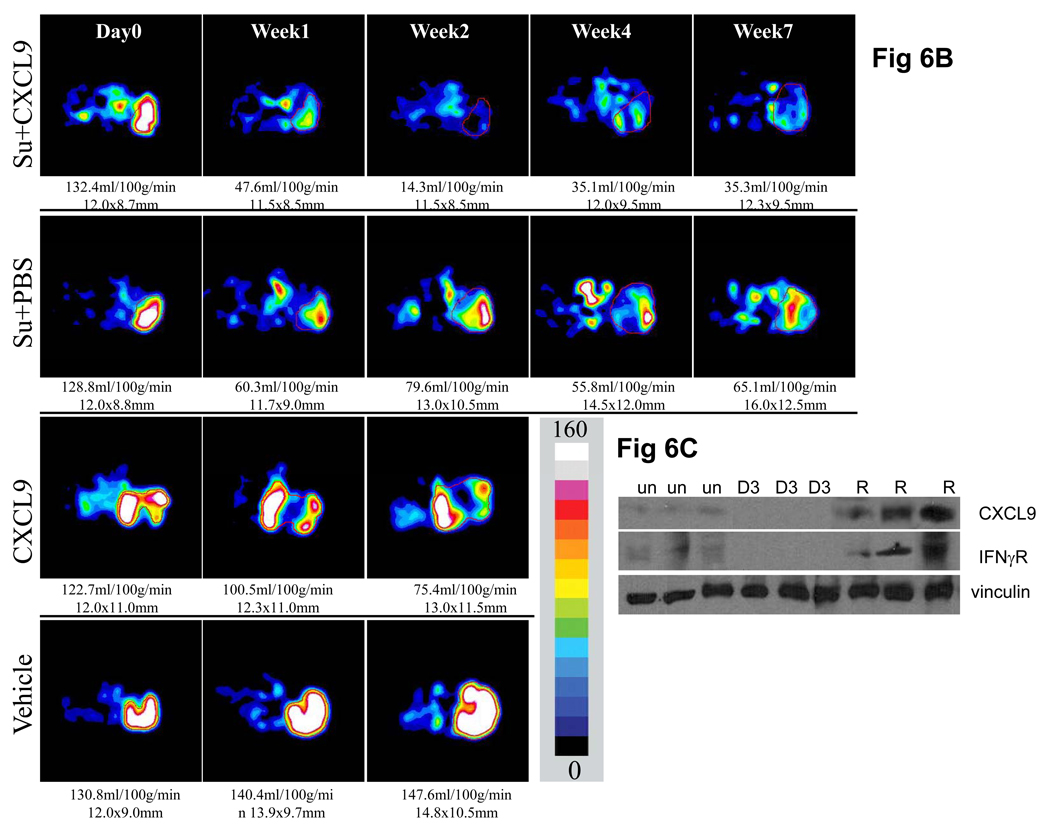
Treatment of metastatic renal cell cancer (RCC) with antiangiogenic agents that block vascular endothelial growth factor (VEGF) receptor 2 signaling produces tumor regression in a substantial fraction of patients; however, resistance typically develops within 6 to 12 months. The purpose of this study was to identify molecular pathways involved in resistance. Treatment of mice bearing either 786-0 or A498 human RCC xenografts with sorafenib or sunitinib produced tumor growth stabilization followed by regrowth despite continued drug administration analogous to the clinical experience. Tumors and plasma were harvested at day 3 of therapy and at the time of resistance to assess pathways that may be involved in resistance. Serial perfusion imaging, and plasma and tumor collections were obtained in mice treated with either placebo or sunitinib alone or in combination with intratumoral injections of the angiostatic chemokine CXCL9. Sunitinib administration led to an early downmodulation of IFNγ levels as well as reduction of IFNγ receptor and downstream angiostatic chemokines CXCL9 to 11 within the tumor. Intratumoral injection of CXCL9, although producing minimal effects by itself, when combined with sunitinib resulted in delayed resistance in vivo accompanied by a prolonged reduction of microvascular density and tumor perfusion as measured by perfusion imaging relative to sunitinib alone. These results provide evidence that resistance to VEGF receptor therapy is due at least in part to resumption of angiogenesis in association with reduction of IFNγ-related angiostatic chemokines, and that this resistance can be delayed by concomitant administration of CXCL9.
Figures
References
-
- Kaelin WG., Jr The von Hippel-Lindau protein, HIF hydroxylation, and oxygen sensing. Biochem Biophys Res Commun. 2005;338:627. - PubMed
-
- Motzer RJ, Michaelson MD, Redman BG, et al. Activity of SU11248, a multitargeted inhibitor of vascular endothelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell carcinoma. J Clin Oncol. 2006;24:16–24. - PubMed
-
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in Patients With Metastatic Renal Cell Carcinoma. JAMA. 2006;295:2516–2524. - PubMed
-
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115–124. - PubMed
-
- Escudier B, Eisen T, Stadler WM, et al. TARGET Study Group. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125–134. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
