

Effect of acute hypoxia on respiratory muscle fatigue in healthy humans
- PMID: 20701769
- PMCID: PMC2929221
- DOI: 10.1186/1465-9921-11-109
Effect of acute hypoxia on respiratory muscle fatigue in healthy humans
Abstract
Background: Greater diaphragm fatigue has been reported after hypoxic versus normoxic exercise, but whether this is due to increased ventilation and therefore work of breathing or reduced blood oxygenation per se remains unclear. Hence, we assessed the effect of different blood oxygenation level on isolated hyperpnoea-induced inspiratory and expiratory muscle fatigue.
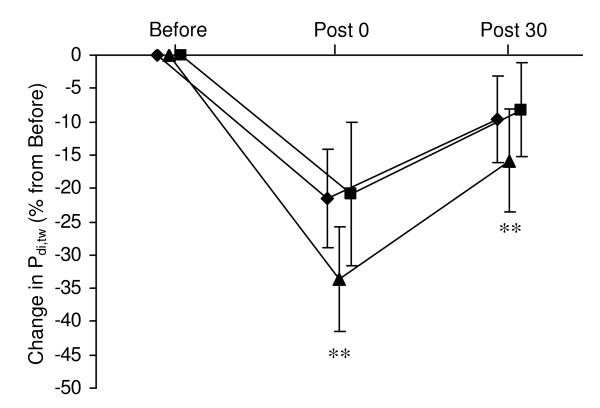
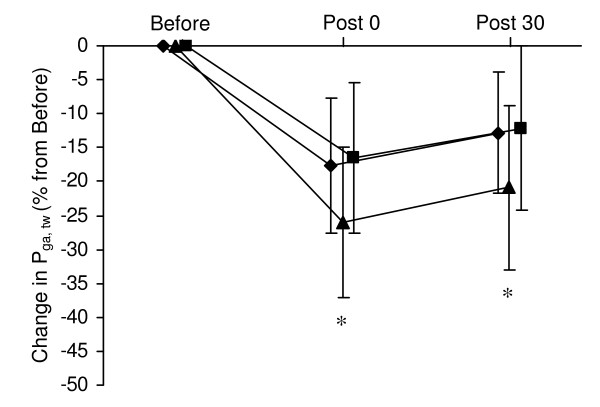
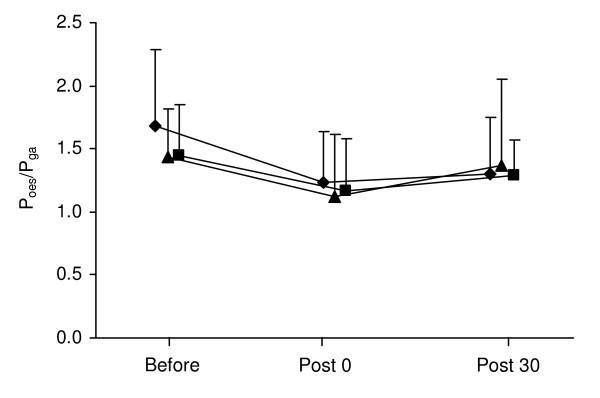
Methods: Twelve healthy males performed three 15-min isocapnic hyperpnoea tests (85% of maximum voluntary ventilation with controlled breathing pattern) in normoxic, hypoxic (SpO2 = 80%) and hyperoxic (FiO2 = 0.60) conditions, in a random order. Before, immediately after and 30 min after hyperpnoea, transdiaphragmatic pressure (P(di,tw)) was measured during cervical magnetic stimulation to assess diaphragm contractility, and gastric pressure (P(ga,tw)) was measured during thoracic magnetic stimulation to assess abdominal muscle contractility. Two-way analysis of variance (time x condition) was used to compare hyperpnoea-induced respiratory muscle fatigue between conditions.
Results: Hypoxia enhanced hyperpnoea-induced P(di,tw) and P(ga,tw) reductions both immediately after hyperpnoea (P(di,tw) : normoxia -22 +/- 7% vs hypoxia -34 +/- 8% vs hyperoxia -21 +/- 8%; P(ga,tw) : normoxia -17 +/- 7% vs hypoxia -26 +/- 10% vs hyperoxia -16 +/- 11%; all P < 0.05) and after 30 min of recovery (P(di,tw) : normoxia -10 +/- 7% vs hypoxia -16 +/- 8% vs hyperoxia -8 +/- 7%; P(ga,tw) : normoxia -13 +/- 6% vs hypoxia -21 +/- 9% vs hyperoxia -12 +/- 12%; all P < 0.05). No significant difference in (di,tw) or P(ga,tw) reductions was observed between normoxic and hyperoxic conditions. Also, heart rate and blood lactate concentration during hyperpnoea were higher in hypoxia compared to normoxia and hyperoxia.
Conclusions: These results demonstrate that hypoxia exacerbates both diaphragm and abdominal muscle fatigability. These results emphasize the potential role of respiratory muscle fatigue in exercise performance limitation under conditions coupling increased work of breathing and reduced O2 transport as during exercise in altitude or in hypoxemic patients.
Figures
References
-
- Calbet JA, Boushel R, Radegran G, Sondergaard H, Wagner PD, Saltin B. Determinants of maximal oxygen uptake in severe acute hypoxia. Am J Physiol Regul Integr Comp Physiol. 2003;284(2):R291–303. - PubMed
-
- Peltonen JE, Rantamaki J, Niittymaki SP, Sweins K, Viitasalo JT, Rusko HK. Effects of oxygen fraction in inspired air on rowing performance. Med Sci Sports Exerc. 1995;27(4):573–579. - PubMed
-
- Richardson RS, Grassi B, Gavin TP, Haseler LJ, Tagore K, Roca J, Wagner PD. Evidence of O2 supply-dependent VO2 max in the exercise-trained human quadriceps. J Appl Physiol. 1999;86(3):1048–1053. - PubMed
-
- Kayser B, Narici M, Binzoni T, Grassi B, Cerretelli P. Fatigue and exhaustion in chronic hypobaric hypoxia: influence of exercising muscle mass. J Appl Physiol. 1994;76(2):634–640. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
