

Equity in access to total joint replacement of the hip and knee in England: cross sectional study
- PMID: 20702550
- PMCID: PMC2920379
- DOI: 10.1136/bmj.c4092
Equity in access to total joint replacement of the hip and knee in England: cross sectional study
Abstract
Objective: To explore geographical and sociodemographic factors associated with variation in equity in access to total hip and knee replacement surgery.
Design: Combining small area estimates of need and provision to explore equity in access to care.
Setting: English census wards.
Subjects: Patients throughout England who needed total hip or knee replacement and numbers who received surgery.
Main outcome measures: Predicted rates of need (derived from the Somerset and Avon Survey of Health and English Longitudinal Study of Ageing) and provision (derived from the hospital episode statistics database). Equity rate ratios comparing rates of provision relative to need by sociodemographic, hospital, and distance variables.
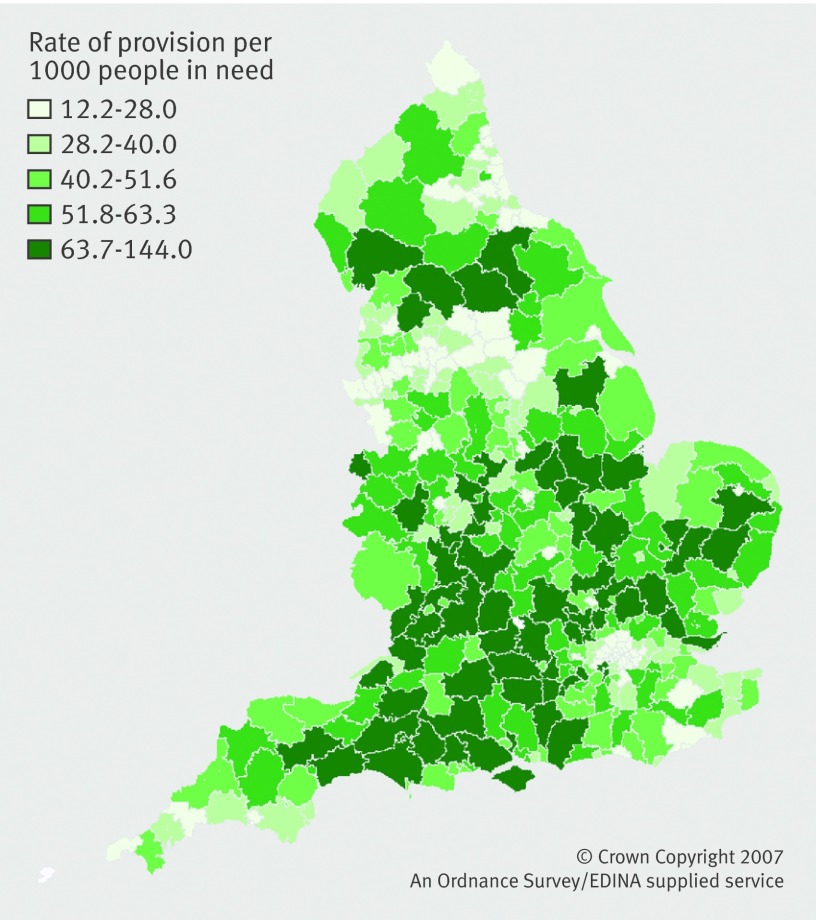
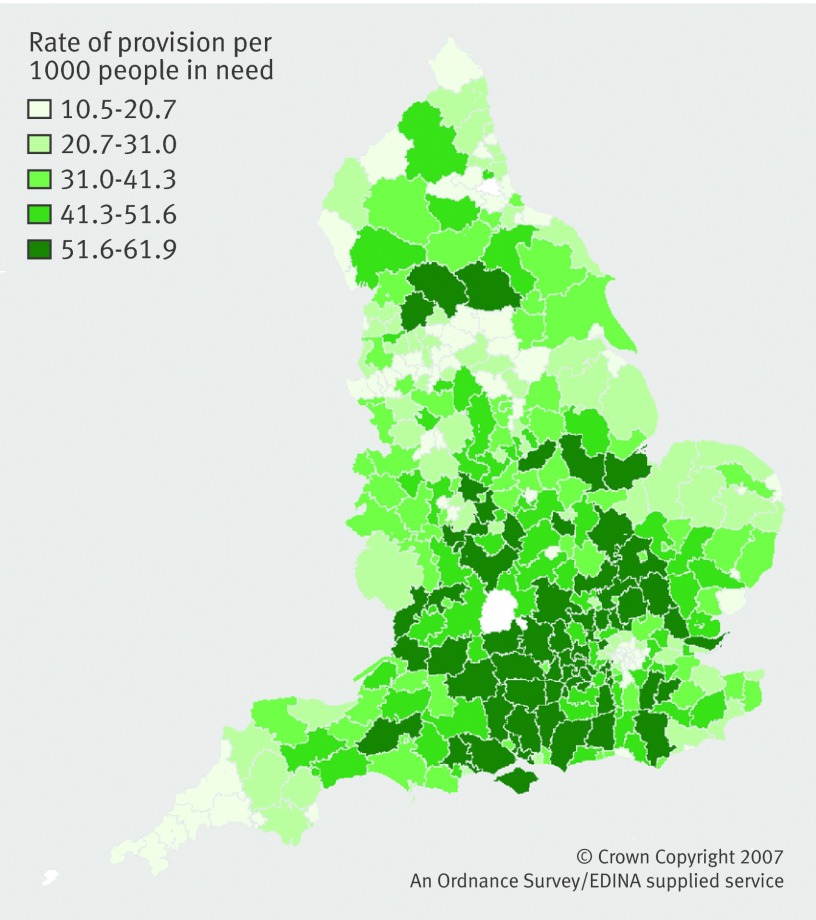
Results: For both operations there was an "n" shaped curve by age. Compared with people aged 50-59, those aged 60-84 got more provision relative to need, while those aged >or=85 received less total hip replacement (adjusted rate ratio 0.68, 95% confidence interval 0.65 to 0.72) and less total knee replacement (0.87, 0.82 to 0.93). Compared with women, men received more provision relative to need for total hip replacement (1.08, 1.05 to 1.10) and total knee replacement (1.31, 1.28 to 1.34). Compared with the least deprived, residents in the most deprived areas got less provision relative to need for total hip replacement (0.31, 0.30 to 0.33) and total knee replacement (0.33, 0.31 to 0.34). For total knee replacement, those in urban areas got higher provision relative to need, but for total hip replacement it was highest in villages/isolated areas. For total knee replacement, patients living in non-white areas received more provision relative to need (1.04, 1.00 to 1.07) than those in predominantly white areas, but for total hip replacement there was no effect. Adjustment for hospital characteristics did not attenuate the effects.
Conclusions: There is evidence of inequity in access to total hip and total knee replacement surgery by age, sex, deprivation, rurality, and ethnicity. Adjustment for hospital and distance did not attenuate these effects. Policy makers should examine factors at the level of patients or primary care to understand the determinants of inequitable provision.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Unequal access to health care in England.BMJ. 2010 Aug 11;341:c3726. doi: 10.1136/bmj.c3726. BMJ. 2010. PMID: 20702549 No abstract available.
-
Access to artificial hips. Using PROMs to improve equity.BMJ. 2010 Sep 15;341:c5014. doi: 10.1136/bmj.c5014. BMJ. 2010. PMID: 20843923 No abstract available.
-
Access to artificial hips. Is still inequitable.BMJ. 2010 Sep 15;341:c5015. doi: 10.1136/bmj.c5015. BMJ. 2010. PMID: 20843924 No abstract available.
Similar articles
-
Geographical variation in the provision of elective primary hip and knee replacement: the role of socio-demographic, hospital and distance variables.J Public Health (Oxf). 2009 Sep;31(3):413-22. doi: 10.1093/pubmed/fdp061. Epub 2009 Jun 19. J Public Health (Oxf). 2009. PMID: 19542267
-
Modeling the need for hip and knee replacement surgery. Part 1. A two-stage cross-cohort approach.Arthritis Rheum. 2009 Dec 15;61(12):1657-66. doi: 10.1002/art.24892. Arthritis Rheum. 2009. PMID: 19950326
-
Modeling the need for hip and knee replacement surgery. Part 2. Incorporating census data to provide small-area predictions for need with uncertainty bounds.Arthritis Rheum. 2009 Dec 15;61(12):1667-73. doi: 10.1002/art.24732. Arthritis Rheum. 2009. PMID: 19950323
-
Revision joint replacement surgeries of the hip and knee across geographic region and socioeconomic status in the western region of Victoria: a cross-sectional multilevel analysis of registry data.BMC Musculoskelet Disord. 2019 Jun 25;20(1):300. doi: 10.1186/s12891-019-2676-z. BMC Musculoskelet Disord. 2019. PMID: 31238918 Free PMC article.
-
Rates of hip and knee joint replacement amongst different ethnic groups in England: an analysis of National Joint Registry data.Osteoarthritis Cartilage. 2017 Apr;25(4):448-454. doi: 10.1016/j.joca.2016.12.030. Epub 2017 Jan 31. Osteoarthritis Cartilage. 2017. PMID: 28159557
Cited by
-
Data Resource Profile: Hospital Episode Statistics Admitted Patient Care (HES APC).Int J Epidemiol. 2017 Aug 1;46(4):1093-1093i. doi: 10.1093/ije/dyx015. Int J Epidemiol. 2017. PMID: 28338941 Free PMC article. No abstract available.
-
Higher Disability in Women Than Men Scheduled for Total Knee Arthroplasty for Degenerative Osteoarthritis: A Cross-Sectional Analysis From India.ACR Open Rheumatol. 2020 Jun;2(6):309-319. doi: 10.1002/acr2.11137. Epub 2020 May 9. ACR Open Rheumatol. 2020. PMID: 32386129 Free PMC article.
-
The pathway to orthopaedic surgery: a population study of the role of access to primary care and availability of orthopaedic services in Ontario, Canada.BMJ Open. 2014 Jul 31;4(7):e004472. doi: 10.1136/bmjopen-2013-004472. BMJ Open. 2014. PMID: 25082417 Free PMC article.
-
How to define responders in osteoarthritis.Curr Med Res Opin. 2013 Jun;29(6):719-29. doi: 10.1185/03007995.2013.792793. Epub 2013 Apr 17. Curr Med Res Opin. 2013. PMID: 23557069 Free PMC article. Review.
-
An ecological study of NHS funded elective hip arthroplasties in England from 2003/04 to 2012/13.J R Soc Med. 2019 Jul;112(7):292-303. doi: 10.1177/0141076819851701. Epub 2019 Jun 6. J R Soc Med. 2019. PMID: 31170358 Free PMC article.
References
-
- Department of Health. On the state of the public health: annual report of the Chief Medical Officer 2005. DH, 2006.
-
- British Medical Association. Healthcare funding review. BMA, 2002.
-
- Department of Health. Tackling health inequalities: status report on the Programme for Action—2006 update on headline indicators. DH 2006.
-
- Department of Health. Health equity audit. A self-assessment tool. DH, 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical