

Cervical and intracranial arterial anomalies in 70 patients with PHACE syndrome
- PMID: 20705698
- PMCID: PMC5967888
- DOI: 10.3174/ajnr.A2206
Cervical and intracranial arterial anomalies in 70 patients with PHACE syndrome
Abstract
Background and purpose: Cerebral and cervical arterial abnormalities are the most common non-cutaneous anomaly in PHACE syndrome, but the location and type of arterial lesions that occur have not been systematically assessed in a large cohort. Our aim was to characterize the phenotypic spectrum of arteriopathy, assess the frequency with which different arteries are involved, and evaluate spatial relationships between arteriopathy, brain structural lesions, and hemangiomas in PHACE syndrome.
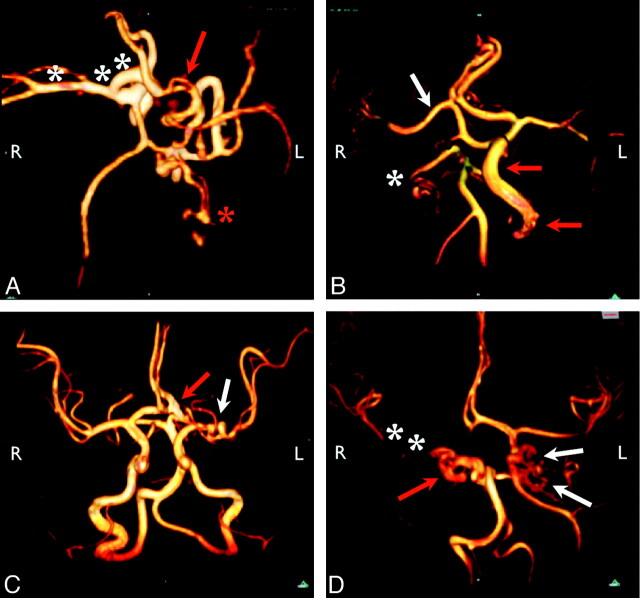
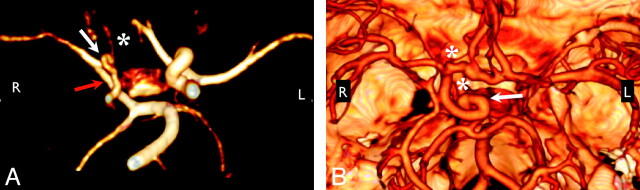
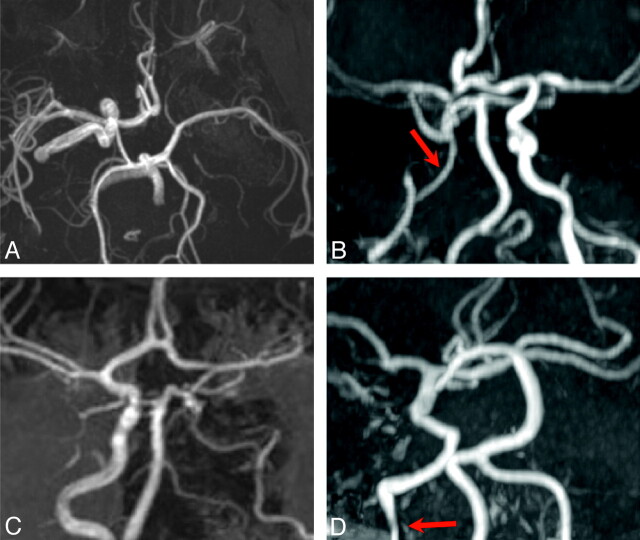
Materials and methods: Intracranial MRA and/or CTA images from 70 children and accompanying brain MR images in 59 patients with arteriopathy and PHACE syndrome were reviewed to identify the type and location of arterial lesions and brain abnormalities. Five categories of arteriopathy were identified and used for classification: dysgenesis, narrowing, nonvisualization, primitive embryonic carotid-vertebrobasilar connections, and anomalous arterial course or origin. Univariate logistic regression analyses were performed to test for associations between arteriopathy location, hemangiomas, and brain abnormalities.
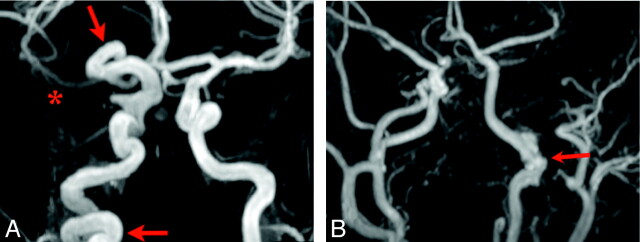
Results: By study design, all patients had arterial abnormalities, and 57% had >1 form of arteriopathy. Dysgenesis was the most common abnormality (56%), followed by anomalous course and/or origin (47%), narrowing (39%), and nonvisualization (20%). Primitive embryonic carotid-vertebrobasilar connections were present in 20% of children. Hemangiomas were ipsilateral to arteriopathy in all but 1 case. The frontotemporal and/or mandibular facial segments were involved in 97% of cases, but no other specific associations between arteriopathy location and hemangioma sites were detected. All cases with posterior fossa anomalies had either ICA anomalies or persistent embryonic carotid-basilar connections.
Conclusions: The arteriopathy of PHACE syndrome commonly involves the ICA and its embryonic branches, ipsilateral to the cutaneous hemangioma, with dysgenesis and abnormal arterial course the most commonly noted abnormalities. Brain abnormalities are also typically ipsilateral.
Figures
References
-
- Frieden IJ, Reese V, Cohen D. PHACE syndrome: the association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch Dermatol 1996;132:302–11 - PubMed
-
- Metry DW, Garzon MC, Drolet BA, et al. PHACE syndrome: current knowledge, future directions. Pediatr Dermatol 2009;26:381–98 - PubMed
-
- Pascual-Castroviejo I. Vascular and nonvascular intracranial malformation associated with external capillary hemangioma. Neuroradiology 1978;16:82–84 - PubMed
-
- Bhattacharya JJ, Luo CB, Álavarez H, et al. PHACES syndrome: a review of eight previously unreported cases with late arterial occlusions. Neuroradiology 2004;46:227–33 - PubMed
-
- Baccin CE, Krings T, Alvarez H, et al. A report of two cases with dolichosegmental intracranial arteries as a new feature of PHACES syndrome. Childs Nerv Syst 2007;23:559–67. Epub 2006 Oct 13 - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous