

Foreskin management: Survey of Canadian pediatric urologists
- PMID: 20705867
- PMCID: PMC2920795
Foreskin management: Survey of Canadian pediatric urologists
Abstract
Objective: To study the approaches to foreskin management of pediatric urologists in Canada.
Design: An online questionnaire comprising several survey questions and clinical vignettes.
Setting: Canada.
Participants: All members of the Pediatric Urologists of Canada.
Main outcome measures: Diagnoses and management strategies for common foreskin conditions seen in consultation, including how many pediatric urologists perform neonatal circumcisions, patient costs, and the reasons for performing the surgery.
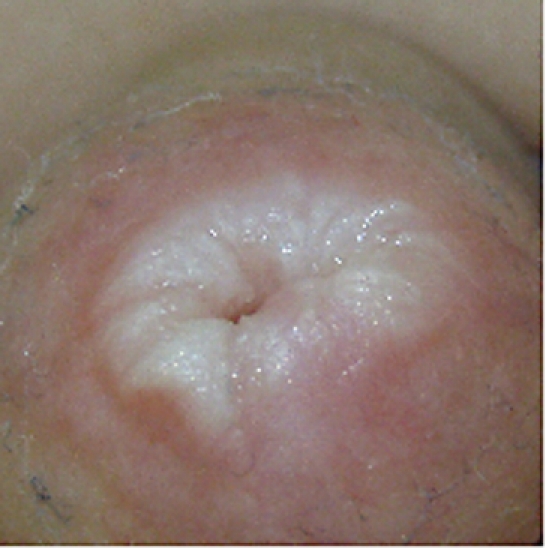
Results: Of the 32 members surveyed, 24 (75%) responded. By far most respondents do not perform neonatal circumcisions; however, many perform circumcisions under general anesthesia for religious and cultural purposes. Typically, patient costs for circumcision range from $500 to $1000. Management of asymptomatic physiologic phimosis is very conservative, with surgeons unlikely to intervene. Neither the presence of ballooning of the foreskin during voiding nor the child's age affects physicians' tendency toward conservative management. Balanitis xerotica obliterans was the only scenario in which most respondents believed there was a need to intervene with either topical steroids or circumcision.
Conclusion: Our data support the hypothesis that pediatric urologists across Canada are very similar in their conservative approach to the management of common foreskin issues. Our goal is to improve the knowledge base among primary care providers and subsequently decrease patient and family anxieties.
OBJECTIF: Examiner les approches adoptées par les urologues pédiatriques au Canada en ce qui concerne la prise en charge des problèmes du prépuce.
TYPE D’ÉTUDE: Questionnaire en ligne comportant diverses questions et vignettes cliniques.
CONTEXTE: Canada.
PARTICIPANTS: Tous les membres des Urologues pédiatriques du Canada.
PRINCIPAUX PARAMÈTRES ÉTUDIÉS: Les diagnostics et les stratégies de prise en charge des problèmes courants du prépuce observés en consultation, y compris le nombre d’urologues pédiatriques qui effectuent des circoncisions néonatales, les frais assumés par les patients et les raisons de la chirurgie.
RÉSULTATS: Des 32 membres sollicités, 24 (75 %) ont répondu. La grande majorité des répondants ne font pas de circoncisions néonatales; par contre, beaucoup le font sous anesthésie générale pour des raisons religieuses et culturelles. Typiquement, les frais de la circoncision varient entre 500 $ et 1 000 $. La prise en charge du phimosis physiologique asymptomatique est très conservatrice, c’est-à-dire que les chirurgiens n’interviendront probablement pas. Ni la présence d’un ballonnement du prépuce durant la miction ni l’âge de l’enfant n’influencent la tendance des médecins à prendre le problème en charge de manière conservatrice. La balanite xérotique oblitérante est le seul scénario où la plupart des répondants croient qu’une intervention est nécessaire au moyen de stéroïdes topiques ou de la circoncision.
CONCLUSION: Nos données corroborent l’hypothèse voulant que les urologues pédiatriques au Canada adoptent une approche conservatrice très semblable dans la prise en charge des problèmes courants du prépuce. Nous avons pour objectif d’approfondir la base de connaissances des médecins de première ligne et d’atténuer ainsi l’anxiété des patients et de leur famille.
Figures



Comment in
-
Gairdner was wrong.Can Fam Physician. 2010 Oct;56(10):986-7. Can Fam Physician. 2010. PMID: 20944034 Free PMC article. No abstract available.
-
Foreskin management.Can Fam Physician. 2010 Oct;56(10):986. Can Fam Physician. 2010. PMID: 20944035 Free PMC article. No abstract available.
References
-
- Foetus and Newborn Committee, Canadian Paediatric Society Circumcision in the newborn period. CPS News Bull Suppl. 1975;8(2):1–2. Available from: www.cirp.org/library/statements/cps1975. Accessed 2010 Jun 22.
-
- American Academy of Pediatrics Task Force on Circumcision Circumcision policy statement. Pediatrics. 1999;103(3):686–93. - PubMed
-
- Hutcheson JC. Male neonatal circumcision: indications, controversies and complications. Urol Clin North Am. 2004;31(3):461–7. viii. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical