

Impact of knee osteoarthritis on health care resource utilization in a US population-based national sample
- PMID: 20706165
- PMCID: PMC3258446
- DOI: 10.1097/MLR.0b013e3181e419b1
Impact of knee osteoarthritis on health care resource utilization in a US population-based national sample
Abstract
Objective: We sought to estimate the impact of knee osteoarthritis (OA) on health care utilization.
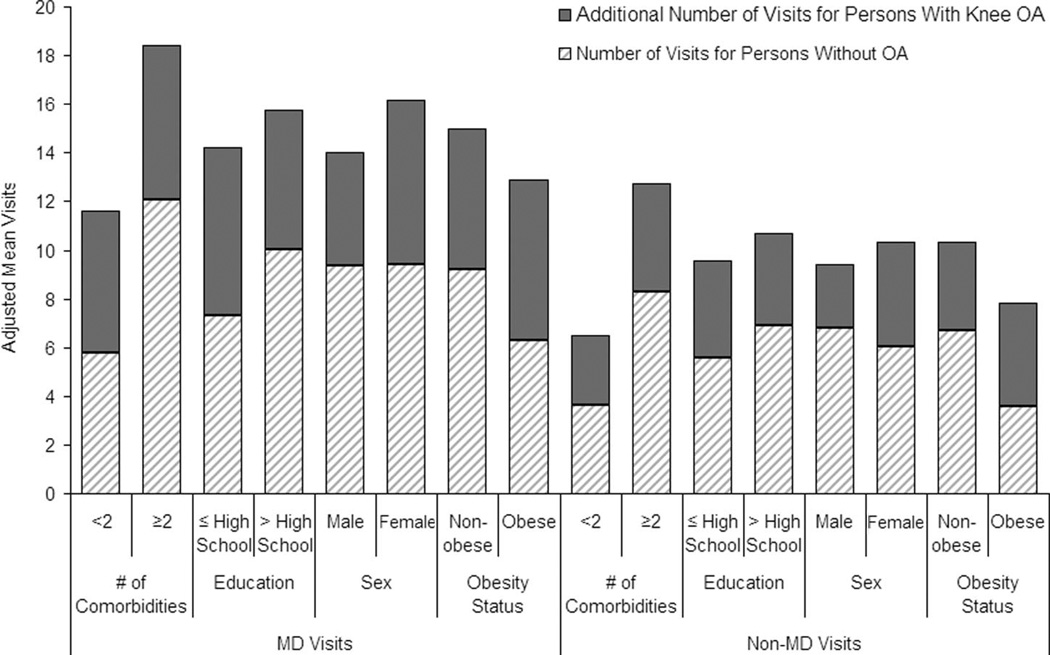
Research design: Using the 2003 Medicare Current Beneficiary Survey, a population-based survey of Medicare beneficiaries linked to Medicare claims, we selected a national cohort of community-dwelling persons aged 65 and older with knee OA and a sex- and age-matched comparison cohort without any form of OA. We distinguished following 4 components of health care utilization: physician (MD) office visits, non-MD office visits, inpatient hospital stays, and emergency department visits. We built multiple regression models to determine whether knee OA affects utilization, controlling for comorbidity count, obesity, functional limitation, education, race, and working status.
Results: A total of 545 Medicare Current Beneficiary Survey participants with knee OA were matched with 1090 OA-free individuals. Mean age in both cohorts was 76 years; approximately 70% were female. Knee OA and OA-free subjects differed significantly in obesity (Knee OA: 37%, OA-free: 20%), % with >or=2 comorbidities (Knee OA: 69%, OA-free: 43%), and functional limitation (Knee OA: 42%, OA-free: 26%). In multivariable regression models, the knee OA cohort had on average 6.0 more annual MD visits (95% confidence interval [CI]: 4.7, 7.4) and 3.8 more non-MD visits (95% CI: 2.8, 4.7) than the OA-free cohort. The knee OA cohort also had 28% more hospital stays (odds ratio [OR] = 1.3, 95% CI: 1.0, 1.6), a difference attributable to total joint replacements.
Conclusions: This first national, population-based study of health care utilization in persons with knee OA documents considerable excess utilization attributable to knee OA, independent of comorbidity, and other patient characteristics.
Figures
References
-
- Dillon CF, Rasch EK, Gu Q, et al. Prevalence of knee osteoarthritis in the United States: arthritis data from the Third National Health and Nutrition Examination Survey 1991–94. J Rheumatol. 2006;33:2271–2279. - PubMed
-
- Breedveld FC. Osteoarthritis—the impact of a serious disease. Rheumatology (Oxford) 2004;43 suppl 1:i4–i8. - PubMed
-
- Reginster JY. The prevalence and burden of arthritis. Rheumatology (Oxford) 2002;41 suppl 1:3–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
