

Giant cell tumor of bone: risk factors for recurrence
- PMID: 20706812
- PMCID: PMC3018195
- DOI: 10.1007/s11999-010-1501-7
Giant cell tumor of bone: risk factors for recurrence
Abstract
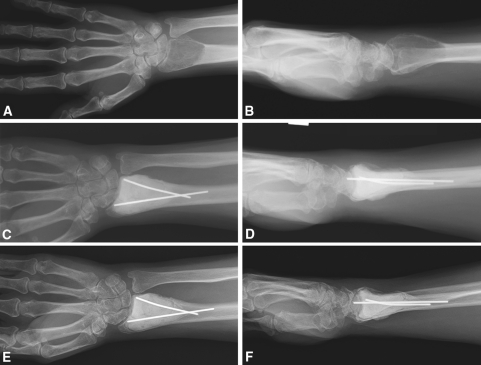
Background: Many surgeons treat giant cell tumor of bone (GCT) with intralesional curettage. Wide resection is reserved for extensive bone destruction where joint preservation is impossible or when expendable sites (eg, fibular head) are affected. Adjuvants such as polymethylmethacrylate and phenol have been recommended to reduce the risk of local recurrence after intralesional surgery. However, the best treatment of these tumors and risk factors for recurrence remain controversial.
Questions/purposes: We evaluated the recurrence-free survival after surgical treatment of GCT to determine the influence of the surgical approach, adjuvant treatment, local tumor presentation, and demographic factors on the risk of recurrence.
Methods: We retrospectively reviewed 118 patients treated for benign GCT of bone between 1985 and 2005. Recurrence rates, risk factors for recurrence and the development of pulmonary metastases were determined. The minimum followup was 36 months (mean, 108.4 ± 43.7; range, 36-233 months).
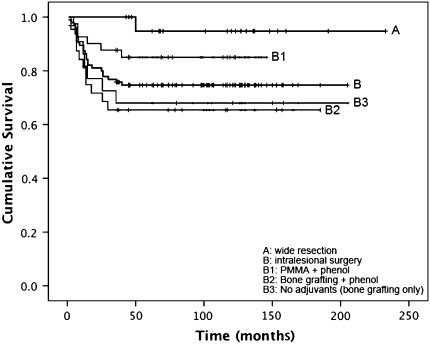
Results: Wide resection had a lower recurrence rate than intralesional surgery (5% versus 25%). Application of polymethylmethacrylate decreased the risk of local recurrence after intralesional surgery compared with bone grafting; phenol application alone had no effect on the risk of recurrence. Pulmonary metastases occurred in 4%; multidisciplinary treatment including wedge resection, chemotherapy, and radiotherapy achieved disease-free survival or stable disease in all of these patients.
Conclusion: We recommend intralesional surgery with polymethylmethacrylate for the majority of primary GCTs. Because pulmonary metastases are rare and aggressive treatment of pulmonary metastases is usually successful, we believe the potential for metastases should not by itself create an indication for wide resection of primary tumors.
Level of evidence: Level III, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures
References
-
- Bertoni F, Present D, Sudanese A, Baldini N, Bacchini P, Campanacci M. Giant-cell tumor of bone with pulmonary metastases: six case reports and a review of the literature. Clin Orthop Relat Res. 1988;237:275–285. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
