

The therapeutic effect of anti-HER2/neu antibody depends on both innate and adaptive immunity
- PMID: 20708157
- PMCID: PMC2923645
- DOI: 10.1016/j.ccr.2010.06.014
The therapeutic effect of anti-HER2/neu antibody depends on both innate and adaptive immunity
Abstract
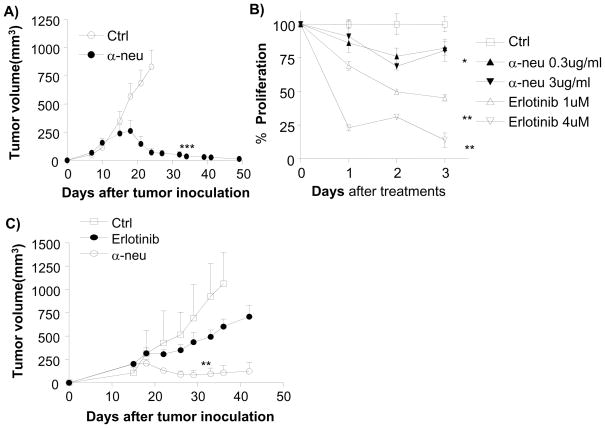
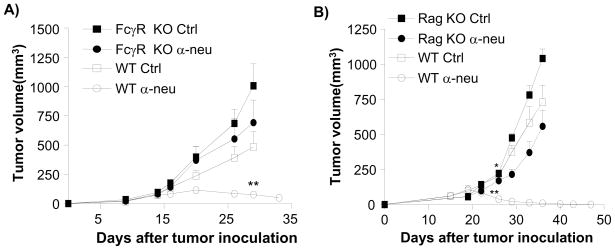
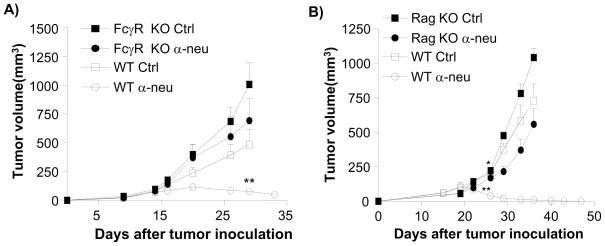
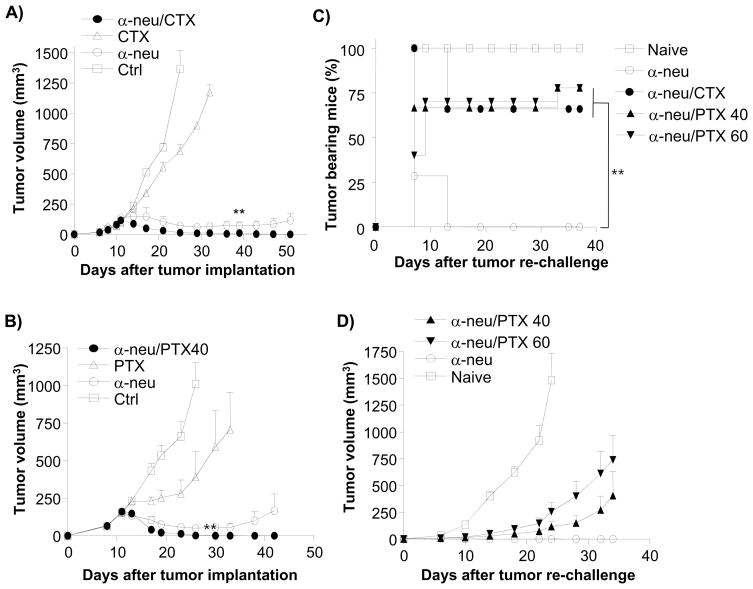
Anti-HER2/neu antibody therapy is reported to mediate tumor regression by interrupting oncogenic signals and/or inducing FcR-mediated cytotoxicity. Here, we demonstrate that the mechanisms of tumor regression by this therapy also require the adaptive immune response. Activation of innate immunity and T cells, initiated by antibody treatment, was necessary. Intriguingly, the addition of chemotherapeutic drugs, although capable of enhancing the reduction of tumor burden, could abrogate antibody-initiated immunity leading to decreased resistance to rechallenge or earlier relapse. Increased influx of both innate and adaptive immune cells into the tumor microenvironment by a selected immunotherapy further enhanced subsequent antibody-induced immunity, leading to increased tumor eradication and resistance to rechallenge. This study proposes a model and strategy for anti-HER2/neu antibody-mediated tumor clearance.
2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures

Comment in
-
Her 2 in 1.Cancer Cell. 2010 Aug 9;18(2):101-2. doi: 10.1016/j.ccr.2010.07.009. Cancer Cell. 2010. PMID: 20708150
References
-
- Aomatsu T, Komatsu H, Yoden A, Hosomi A, Miyazaki H, Sogo T, Inui A, Fujisawa T, Tamai H. Fulminant hepatitis B and acute hepatitis B due to intrafamilial transmission of HBV after chemotherapy for non-Hodgkin's lymphoma in an HBV carrier. Eur J Pediatr. 2010;169:167–171. - PubMed
-
- Apetoh L, Ghiringhelli F, Tesniere A, Obeid M, Ortiz C, Criollo A, Mignot G, Maiuri MC, Ullrich E, Saulnier P, et al. Toll-like receptor 4-dependent contribution of the immune system to anticancer chemotherapy and radiotherapy. Nat Med. 2007;13:1050–1059. - PubMed
-
- Burgdorf S, Scholz C, Kautz A, Tampe R, Kurts C. Spatial and mechanistic separation of cross-presentation and endogenous antigen presentation. Nat Immunol. 2008;9:558–566. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
