

Contemporary cesarean delivery practice in the United States
- PMID: 20708166
- PMCID: PMC2947574
- DOI: 10.1016/j.ajog.2010.06.058
Contemporary cesarean delivery practice in the United States
Abstract
Objective: To describe contemporary cesarean delivery practice in the United States.
Study design: Consortium on Safe Labor collected detailed labor and delivery information from 228,668 electronic medical records from 19 hospitals across the United States, 2002-2008.
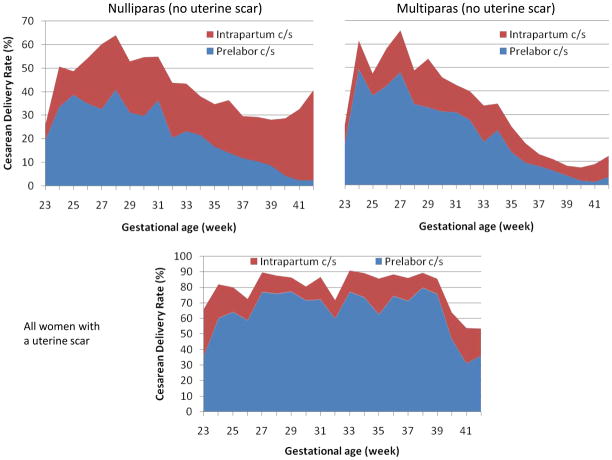
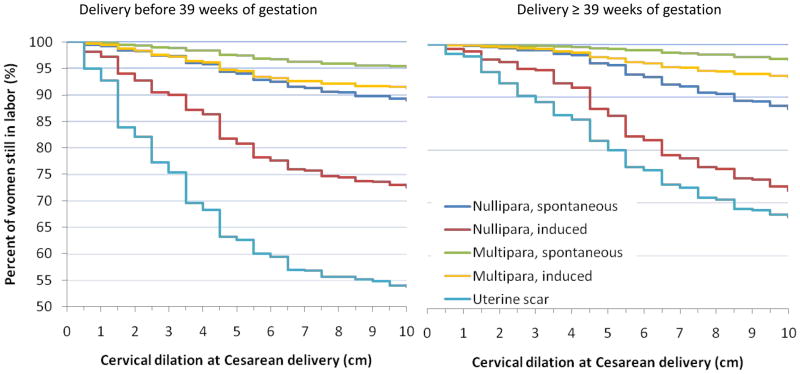
Results: The overall cesarean delivery rate was 30.5%. The 31.2% of nulliparous women were delivered by cesarean section. Prelabor repeat cesarean delivery due to a previous uterine scar contributed 30.9% of all cesarean sections. The 28.8% of women with a uterine scar had a trial of labor and the success rate was 57.1%. The 43.8% women attempting vaginal delivery had induction. Half of cesarean for dystocia in induced labor were performed before 6 cm of cervical dilation.
Conclusion: To decrease cesarean delivery rate in the United States, reducing primary cesarean delivery is the key. Increasing vaginal birth after previous cesarean rate is urgently needed. Cesarean section for dystocia should be avoided before the active phase is established, particularly in nulliparous women and in induced labor.
Published by Mosby, Inc.
Figures
References
-
- Villar J, Valladares E, Wojdyla D, et al. Caesarean delivery rates and pregnancy outcomes: the 2005 WHO global survey on maternal and perinatal health in Latin America. Lancet. 2006 Jun 3;367(9525):1819–29. - PubMed
-
- Lumbiganon P, Laopaiboon M, Gülmezoglu AM, et al. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007–08. Lancet. 2010;375(9713):490–9. - PubMed
-
- Hamilton BE, Martin JA, Ventura SJ. National vital statistics reports, Web release. 12. Vol. 57. Hyattsville, MD: National Center for Health Statistics; Births: Preliminary data for 2007. Released March 18, 2009.
-
- Joseph KS, Young DC, Dodds L, O’Connell CM, Allen VM, Chandra S, Allen AC. Changes in maternal characteristics and obstetric practice and recent increases in primary cesarean delivery. Obstet Gynecol. 2003;102:791–800. - PubMed
-
- Macones GA. Clinical outcomes in VBAC attempts: what to say to patients? Am J Obstet Gynecol. 2008;199:1–2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
