

Pancreatic cancer tumor size on CT scan versus pathologic specimen: implications for radiation treatment planning
- PMID: 20708856
- PMCID: PMC4362517
- DOI: 10.1016/j.ijrobp.2010.04.058
Pancreatic cancer tumor size on CT scan versus pathologic specimen: implications for radiation treatment planning
Abstract
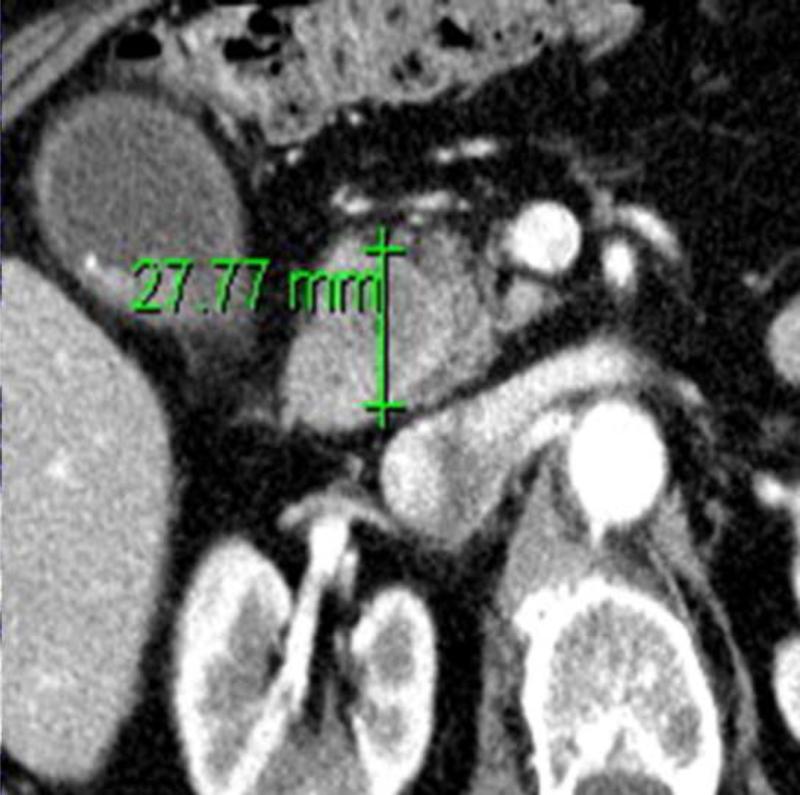
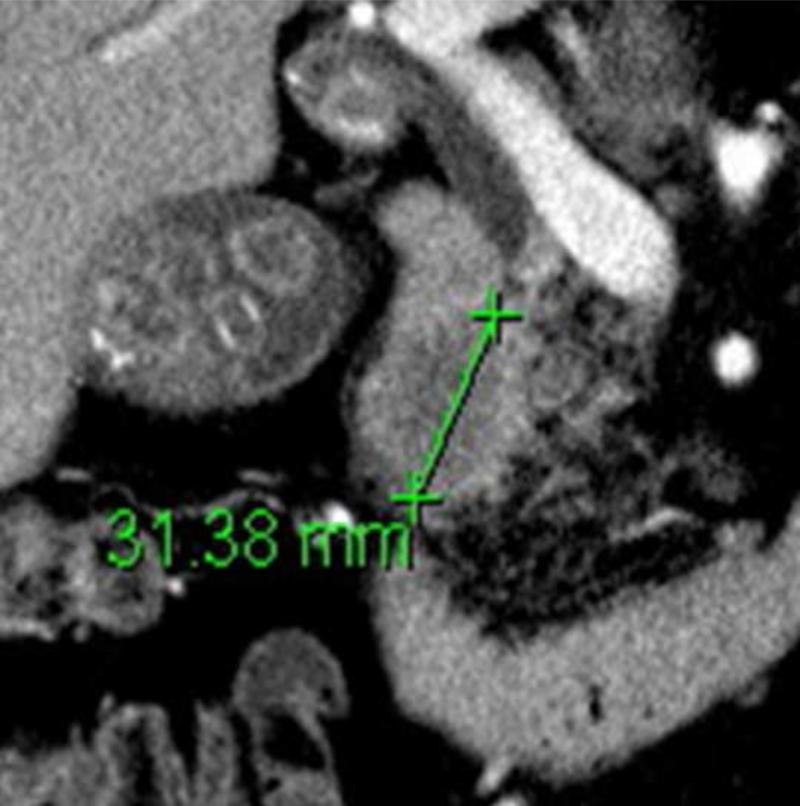
Purpose: Pancreatic cancer primary tumor size measurements are often discordant between computed tomography (CT) and pathologic specimen after resection. Dimensions of the primary tumor are increasingly relevant in an era of highly conformal radiotherapy.
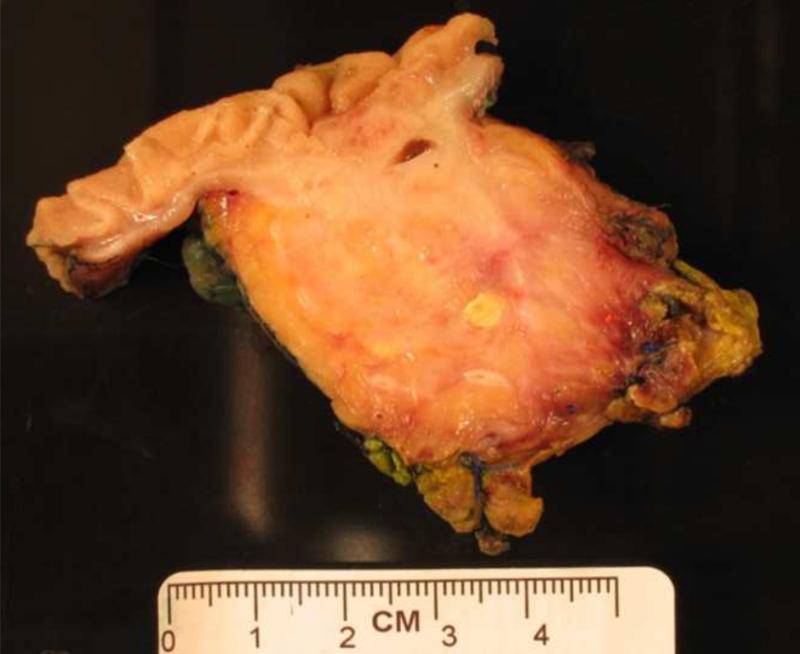
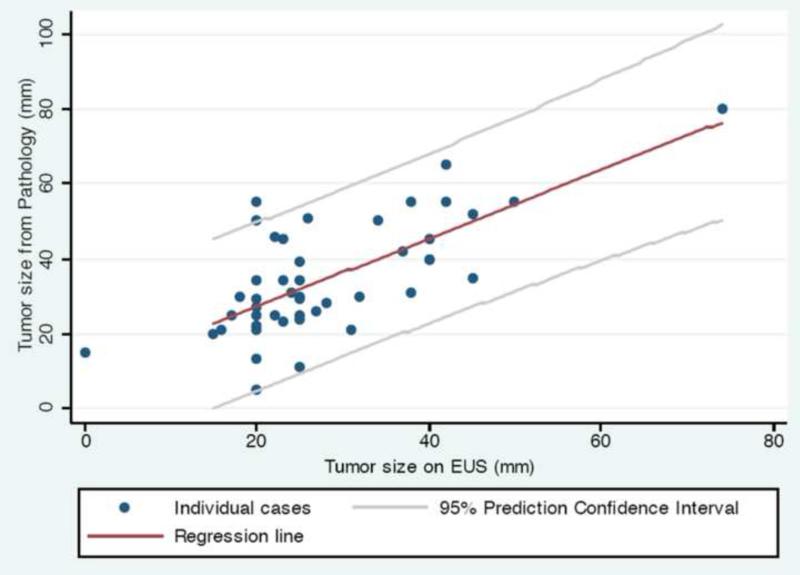
Methods and materials: We retrospectively evaluated 97 consecutive patients with resected pancreatic cancer at two Boston hospitals. All patients had CT scans before surgical resection. Primary endpoints were maximum dimension (in millimeters) of the primary tumor in any direction as reported by the radiologist on CT and by the pathologist for the resected gross fresh specimen. Endoscopic ultrasound (EUS) findings were analyzed if available.
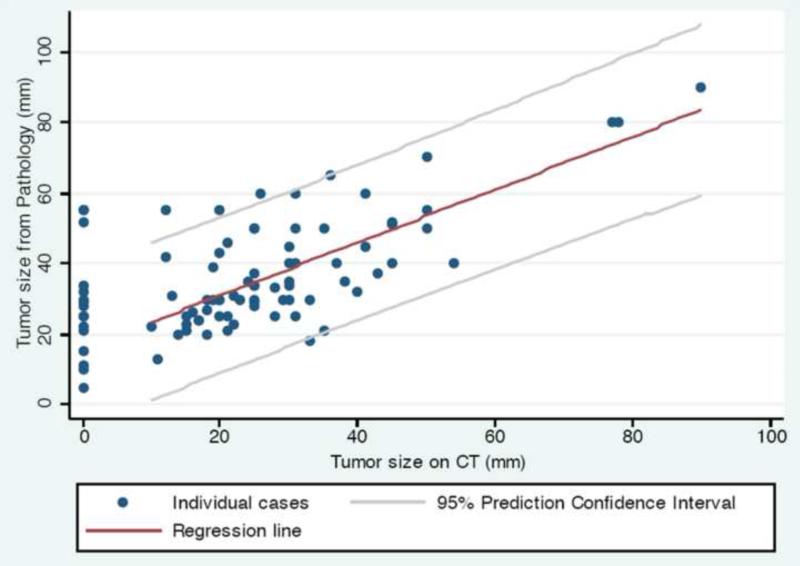
Results: Of the patients, 87 (90%) had preoperative CT scans available for review and 46 (47%) had EUS. Among proximal tumors (n = 69), 40 (58%) had pathologic duodenal invasion, which was seen on CT in only 3 cases. The pathologic tumor size was a median of 7 mm larger compared with CT size for the same patient (range, -15 to 43 mm; p < 0.0001), with 73 patients (84%) having a primary tumor larger on pathology than CT. Endoscopic ultrasound was somewhat more accurate, with pathologic tumor size being a median of only 5 mm larger compared with EUS size (range, -15 to 35 mm; p = 0.0003).
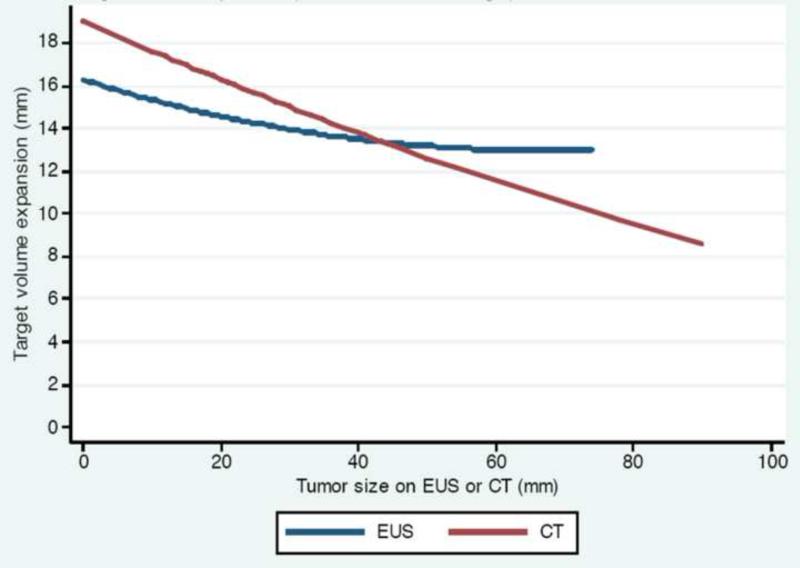
Conclusions: Computed tomography scans significantly under-represent pancreatic cancer tumor size compared with pathologic specimens in resectable cases. We propose a clinical target volume expansion formula for the primary tumor based on our data. The high rate of pathologic duodenal invasion suggests a risk of duodenal under-coverage with highly conformal radiotherapy.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225. - PubMed
-
- Griffin JF, Smalley SR, Jewell W, et al. Patterns of failure after curative resection of pancreatic carcinoma. Cancer. 1990;66:56–61. - PubMed
-
- Van den Broeck A, Sergeant G, Ectors N, et al. Patterns of recurrence after curative resection of pancreatic ductal adenocarcinoma. Eur J Surg Oncol. 2009;35:600–604. - PubMed
-
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg. 1985;120:899–903. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
