

Principles of cancer screening: lessons from history and study design issues
- PMID: 20709205
- PMCID: PMC2921618
- DOI: 10.1053/j.seminoncol.2010.05.006
Principles of cancer screening: lessons from history and study design issues
Abstract
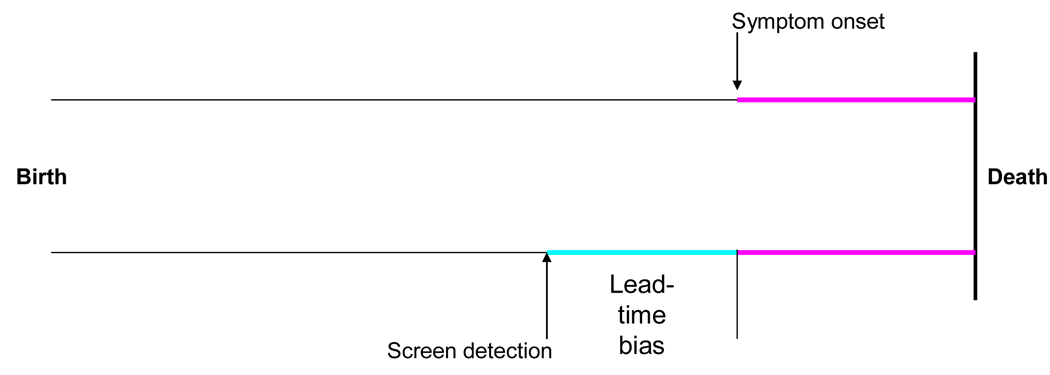
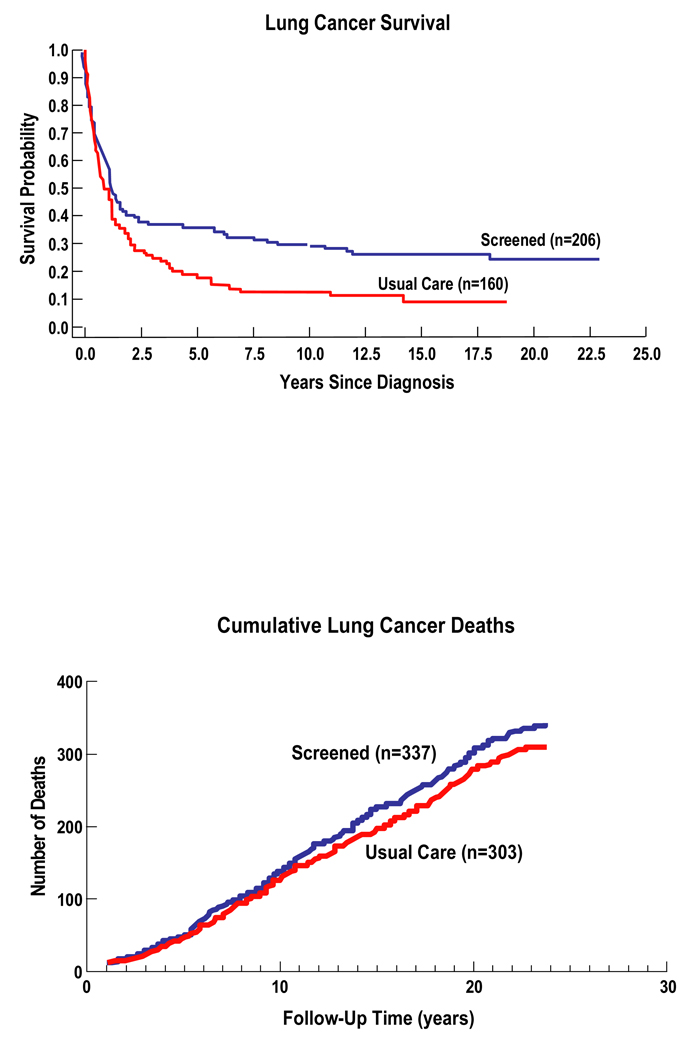
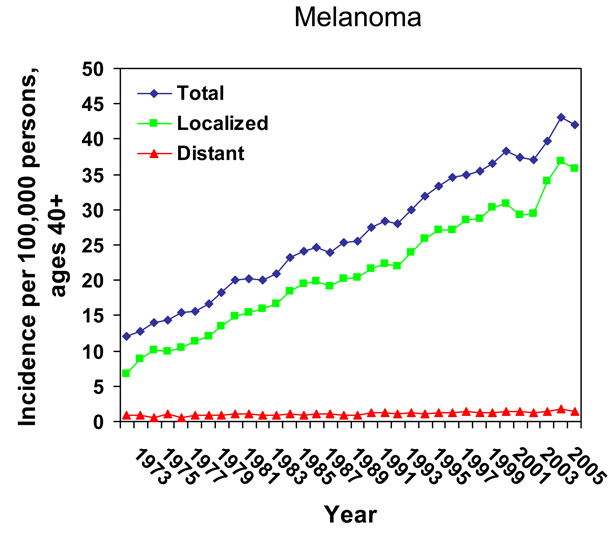
Early detection of cancer has held great promise and intuitive appeal in the medical community for well over a century. Its history developed in tandem with that of the periodic health examination, in which any deviations--subtle or glaring--from a clearly demarcated "normal" were to be rooted out, given the underlying hypothesis that diseases develop along progressive linear paths of increasing abnormalities. This model of disease development drove the logical deduction that early detection, by "breaking the chain" of cancer development, must be of benefit to affected individuals. In the latter half of the 20th century, researchers and guidelines organizations began to explicitly challenge the core assumptions underpinning many clinical practices. A move away from intuitive thinking began with the development of evidence-based medicine. One key method developed to explicitly quantify the overall risk-benefit profile of a given procedure was the analytic framework. The shift away from pure deductive reasoning and reliance on personal observation was driven, in part, by a rising awareness of critical biases in cancer screening that can mislead clinicians, including healthy volunteer bias, length-biased sampling, lead-time bias, and overdiagnosis. A new focus on the net balance of both benefits and harms when determining the overall worth of an intervention also arose: it was recognized that the potential downsides of early detection were frequently overlooked or discounted because screening is performed on basically healthy persons and initially involves relatively noninvasive methods. Although still inconsistently applied to early detection programs, policies, and belief systems in the United States, an evidence-based approach is essential to counteract the misleading--even potentially harmful--allure of intuition and individual observation.
Published by Elsevier Inc.
Figures


References
-
- Han PK. Historical changes in the objectives of the periodic health examination. Ann Intern Med. 1997;127(10):910–917. - PubMed
-
- Boulware LE, Barnes GJ, Wilson RF, et al. Value of the Periodic Health Evaluation. Evidence Report/Technology Assessment No. 136. (Prepared by The Johns Hopkins University Evidence-based Practice Center under Contract No. 290-02-0018) Rockville, MD: Agency for Healthcare Research and Quality; 2006. Apr, AHRQ Publication No. 06-E011.
-
- Dobell H. Lectures on the Germs and Vestiges of Disease, and on the Prevention of the Invasion and Fatality of Disease by Periodical Examinations. London: Churchill; 1861.
-
- Gould GM. A system of personal biologic examinations the condition of adequate medical and scientific conduct of life. JAMA. 1900;284:134–138. - PubMed
-
- Childe CP. The Control of a Scourge, or How Cancer is Curable. New York: E.P. Dutton & Company; 1907.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
